Implant dentistry is a vast and detailed dental specialty. Patients desire a lifelike, esthetic implant, and clinicians want an implant that isn’t going to be a huge inconvenience to place. The best answer: immediate implant placement or loading.
Traditionally, there is a designated amount of time between tooth extraction and implant placement, but immediate loading reduces that time and allows the surgeon to place the implant close to the time of extraction. When immediately loading implants, this can happen in a short amount of time, versus the standard of 2 to 3 months for traditionally placed implants in the mandible or 4 to 6 months in the maxilla.1-2 As one can imagine, this is a huge benefit for patients who don’t want to be edentulous for months for both esthetic and functional reasons. A 2014 survey demonstrated that patients preferred this type of treatment over any other implant procedure.3
“Initially, clinicians would expose the bone, place the implant, close the flap, let it heal for 3 months, then open the flap again and complete the prosthesis using an abutment and a crown. This process could take 6 to 9 months,” says Indraneel Kanaglekar, senior vice president and president of global dental for ZimVie, a company that offers end-to-end tooth replacement solutions such as implants, biomaterials, and digital workflow solutions. “Now with technological advancements, you can do a flapless surgery to place and restore an implant immediately.”
So why wouldn’t a clinician immediately place implants for every patient? If it is so convenient and cuts down on time for both patient and practitioner, why isn’t it the standard? There are several stipulations and requirements that the patient must meet before they are considered for this type of placement, according to Scott McNally, vice president of sales (Eastern US and Canada) for MegaGen America.
“You have to look at the medications the patient is on, the surface technology, how many implants you’re placing,” McNally says. “Maybe in 1 situation you can predictably load an implant in 8 weeks, but that doesn’t mean that will be the case for everybody. We must look at how it will affect the patient for the long term.”
To better understand the workflow for immediately placing implants and how to succeed with it, it helps to know the background of the procedure, and implants as a whole.
The History of Immediate Loading Implants
The popularization of successful titanium implant placement in 1965 was done by Swedish professor and researcher Per-Ingvar Brånemark, MD, PhD. Immediately loading implants were first demonstrated in the late 1970s, coming onto the scene as the Tübingen immediate implant, named for a university city in Germany.4 These early immediately loading implants were stable, though success often hinged on patient adherence and careful treatment considerations.4
A few years after that first immediate placement, Joel Rosenlicht, DMD, an oral and maxillofacial surgeon who later became president of the American Academy of Implant Dentistry, used immediate loading implants in his implant practice from the start. Dr Rosenlicht is the advisory board chairman for Ditron.
“The first implants that I ever placed, back in the early 1980s, were immediately loaded implants. We got involved very early on in a system out of Switzerland that was designed by the International Team for Implantology (Straumann),” Dr Rosenlicht says. “They had a system called the Titanium Plasma Sprayed screw.…The system was designed so that you place 4 implants in the anterior mandible, and then you immediately loaded those 4 implants with the patient’s denture. You converted that denture that day or within a very, very short period of time after the implants were placed. So that denture would be supported by the 4 implants that you placed, and they were highly, highly successful.”
The concept of immediately placed implants is not a new one. Modern technology and biological understanding has helped both restorative dentists and implant surgeons avoid problems that had resulted in implant failure when doing immediately loaded implant procedures in the past.
Small Diameter Implants by Richard Lipscomb Jr, DDS
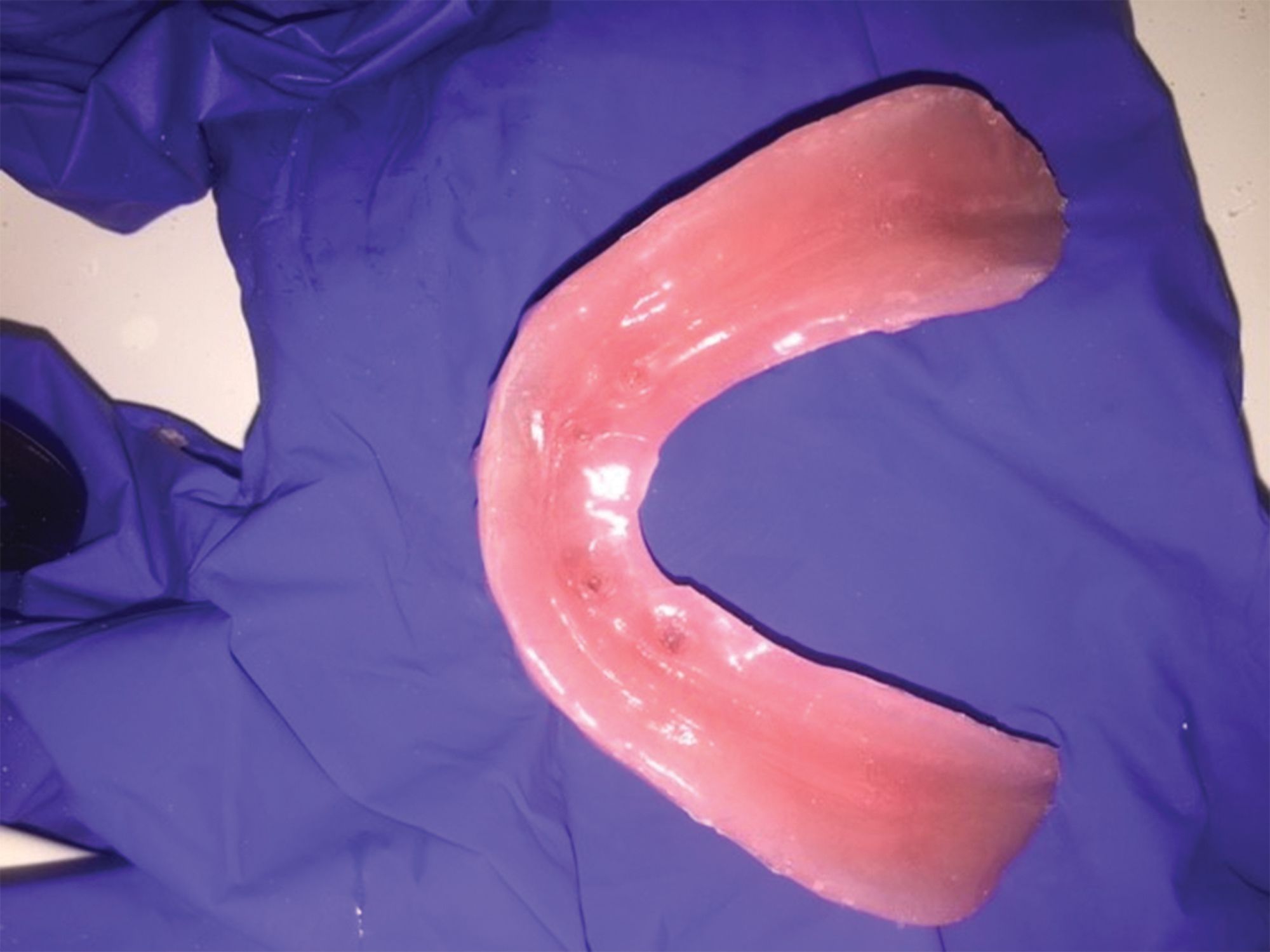
Immediate loading doesn’t always mean permanent loading when it comes to small diameter implants (SDIs). Most dental implants, including SDIs, need a period of time to allow for bone integration, which stabilizes dental implants. Minimizing the occlusal forces being applied to SDIs for the first 3 to 4 months is critical to the implant’s success. There are several ways SDIs can be immediately loaded and still have the support of the surrounding hard and soft tissues. In cases where overdentures are retained by SDI, immediate loading with soft reline materials has its benefits.
The SDIs were placed, the inside of the denture was relieved, and soft reline material was used to buffer the occlusal forces around the implant while aiding in the retention of the overdenture. This technique allows the implants to integrate into a less stressful environment (Figure 1).
When SDIs are used in crown and bridge applications to retain crowns, controlling the occlusal forces is essential for the implants’ survival. In this case, an SDI is replacing tooth #7. The implant abutment is inserted with a silicone shim, while a cotton pellet is tucked into the top of the shim. This will allow for a temporary crown for tooth #7 to be fabricated without touching the abutment of the implant (Figure 2).
The provisional crown is fabricated over the shim and cotton pellet. Once the provisional crown is finished and polished, it’s bonded into place with flowable composite at the interproximal contacts (Figure 3).
The cross-sectional view of the provisional crown and its relationship to the shim and cotton pellet are noted. There is a small space between the top of the shim and the crown that was noted. The lateral forces are neutralized by the shim, the occlusal forces are reduced by the space above the shim, and the SDI is free of stress for the next 3 to 4 months.
Like traditionally sized implants, working with SDIs requires precision and stability, but doing it the right way can result in great, esthetic results for patients.7
Reference
7. Jackson BJ. Small-diameter implants: a 7-year retrospective study. J Oral Implantol. 2017;43(2):125-129. doi:10.1563/aaid-joi-D-16-00098
“What’s happened is we now understand what contributes to failure. So we can minimize the failures that we have in doing immediate load, or these more advanced procedures. We understand what is necessary to make these cases highly predictable and successful—working not only on healthy patients in a healthy environment but [also] recognizing how important stability is,” Dr Rosenlicht says.
Stability is the key factor in every dental implant procedure, not just the immediate placement, Dr Rosenlicht notes.
“When placing an implant that is to be immediately, provisionally, or fully loaded, it is important to understand that a critical principle is that the implant and the restoration are within the physiologic limits of bone healing and maturation,” he says. “For this reason, new implant designs are developed to maximize implant stability and promote more rapid integration as well as an ease for the fabrication and placement of the initial restoration.”
Where Do We Go From Here?
Patients trust clinicians to make the best decisions regarding their health and well-being, and implant dentistry is no exception. Providers should approach each case with care, which includes understanding if a case requires immediate implant loading or the more traditional delayed implant loading.
Although patients may desire the immediate convenience of an immediate loading implant, there are important considerations, per results of a 2015 study in the National Journal of Maxillofacial Surgery.5
“In comparison [with] conventional implant treatment, the immediate loading procedure requires more chairside time at the time of implant placement for both the restorative dentist and the patient. Careful patient screening and selection are required when an immediate implant placement with immediate loading procedure is a treatment consideration,” the study’s authors wrote. “The ideal state for immediately loaded implants would include adequate bone quality (D2 or D3 bone), screw-shaped implants, rough implant surface, minimum implant length of 10 mm, adequate primary stability, and avoidance of lateral forces. Primary stability of immediately placed implant seems to be the most important factor in immediate loading.”
That is all to say that patients need to be adequately observed to determine if they are suitable for this kind of implant placement. As mentioned by Dr Rosenlicht, primary stability is the key factor when considering what type of implant placement will work best for these patients.
Each patient requires specific consideration, particularly regarding implant cases and care. The clinician’s best path forward, may not always be immediate loading implants. “One of the most disappointing things patients experience is going through a surgical procedure like this,” Dr Rosenlicht says, “then having a complication that requires removal from a failure, and then waiting the whole time for everything to heal and to go through the process a second time.”
Timeline of Dental Implants
600 AD - Gems and Metal
Ancient civilizations used ivory, gems, metals, and other materials to replace missing teeth. For instance, the ancient Mayan civilization in Central America used shells to craft dental implants. Although these were hardly the esthetics we expect in the modern day, they functioned for ancient peoples in decorative ways as well as everyday use.
1700s - Gold Alloy
Dentists used gold alloy to create implant teeth. This was not always a realistic option as gold became more valuable, preventing many individuals from receiving the dental care that they needed. Although dental care was more widely available to individuals with more money, it was still incumbent on dental professionals to do intensive implant surgery to make this gold alloy work, costing time and money for results that weren’t esthetic or durable.
1800s - Silver and Porcelain
Following the trend of using metals for dental implants, many prosthodontists began using silver. Silver, much like gold, was not durable and not esthetic. Porcelain was another option for dental professionals, and although it was more esthetic than dark silvers and golds, it did not optimally integrate with the bone. This would lead to further problems down the line.
1900s - Titanium
The rise of modern technologies and the increased focus on scientific research allowed the act of placing dental implants to be a more accessible and understandable procedure. In 1965, Per-Ingvar Brånemark, MD, PhD, successfully placed a titanium dental implant, achieving osseointegration while saving money for dental practices across the world.
1976 - Immediate Load8
In Tübingen, Germany, clinicians began placing dental implants within 48 hours of tooth extraction, making these some of the first recorded cases of immediate loading implants. This procedure and subsequent study demonstrated that, under the right circumstances, clinicians could circumvent the monthslong waiting period and could place implants in less than a week.
Reference
8. Abraham CM. A brief historical perspective on dental implants, their surface coatings and treatments. Open Dent J. 2014;8:50-55. doi:10.2174/1874210601408010050
A standard, delayed loading implant situation typically takes time, resources, and a plan to keep the patient satisfied as they await the final restoration.
“When we have a situation where the patient is healthy, and the environment to which the tooth that’s being either removed or has been removed is also healthy, and the tooth removal is atraumatic, we consider doing immediately loaded implants,” Dr Rosenlicht says. “At that point we can consider placing an immediate implant with a provisional restoration as long as we have enough stability for that implant to heal under controlled occlusal function.”
Provisionally loading an implant allows the patient to have a functional and esthetic temporary restoration as they await their final restoration/implant. The provisionally loaded implant or implants allows the clinician to work in a controlled environment, and the patient now has an opportunity to evaluate how their final restoration may look and feel. Placing immediate implants oftentimes has a significant benefit in preserving existing bone and soft-tissue relationships that can often maximize esthetics.
Immediate loading implants are particularly appealing in cases of esthetic importance where patients’ teeth may be the most visible. Patients don’t want to have to wait for months with a tooth that doesn’t look natural or to have the esthetics they desire. They can also be applicable for cases with fixed prostheses in the maxilla or fixed/removable systems in the mandible.
Another big advantage is the elimination of soft tissue loss that can be associated with implant placement procedures, according to Dr Rosenlicht.
“One of the nice things about placing implants and restorations immediately is that it allows you to support and maintain the existing soft tissue in such a way that it’s not affected by healing in that area without a tooth, or a restoration in place. When a the tooth is removed, there’s what we call remodeling of that bone and soft tissue during that healing process. And often times, soft tissue is lost during that process,” he says. “If we can place an implant, make sure that implant is stable, place a crown, that can support all the soft tissue that’s already there so that doesn’t remodel, we don’t lose it. This can sometimes optimize the esthetics and make the patient more comfortable during the healing phases of these implants. Because there’s nothing removable, temporary, or any space that’s left there with the implant that’s been submerged to go on to heal.”
Dr Rosenlicht says that although single tooth immediate restorations are popular, what has really worked well with this type of implant loading procedure is fully edentulous cases because of cross arch stabilization.
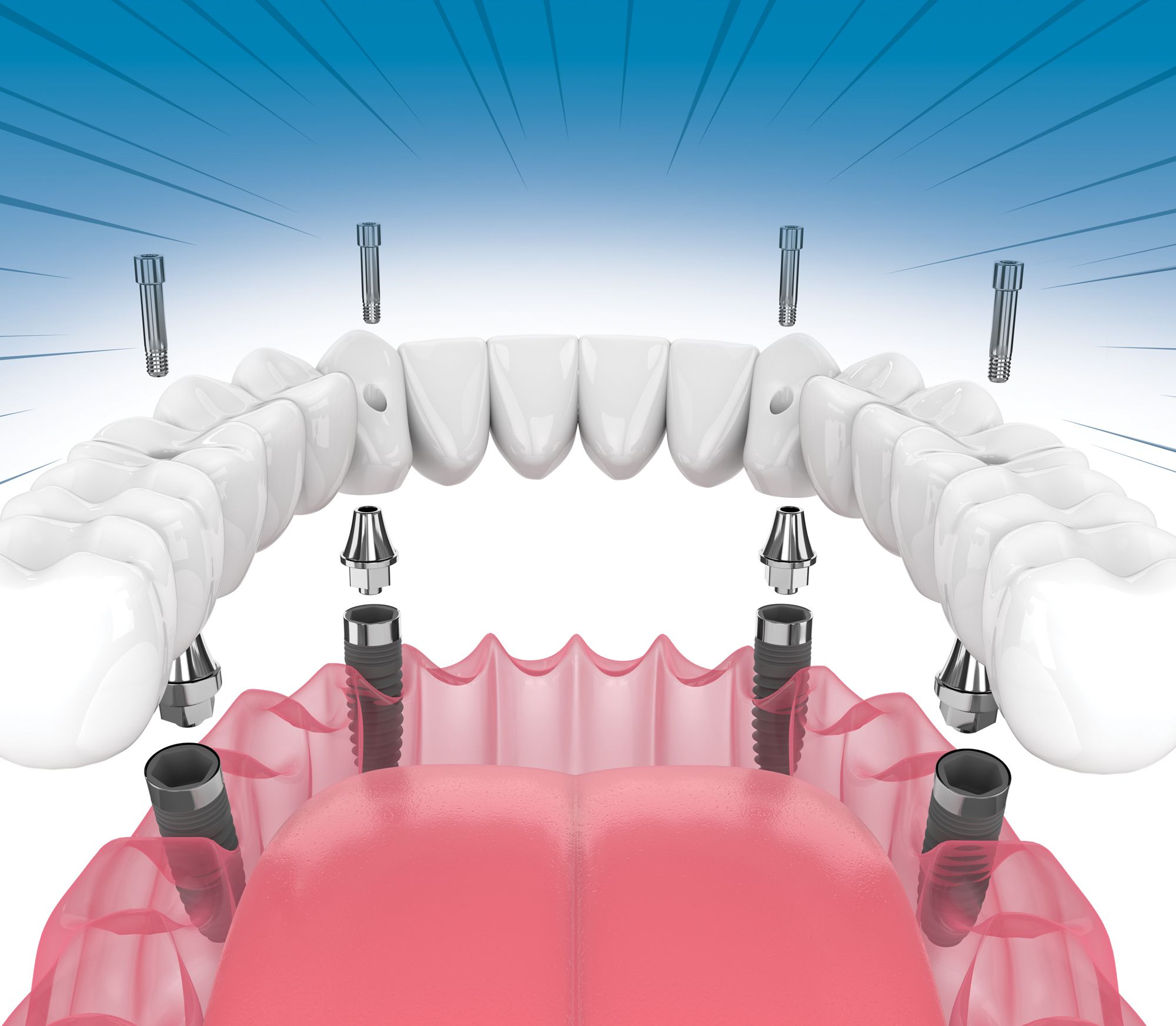
“The All-on-4, All-on-5, [and] All-on-6 concepts have been around a long time and are highly successful. One of the reasons why multiple implants can be loaded immediately, with a lot more assurance that they’ll be successful, is the fact that we now have what we call cross arch stabilization,” he says.
Cross arch stabilization is a key to the All-on-4 solution of a total arch. It ensures that patients will leave on the same day with the support and stability they need to protect the implants during the period of integration. The key concept is that the implants are passively connected and rigidly supported by the superstructure protecting the implants from being overloaded.6
“We’re rigidly connecting these implants passively so that they’re allowed to then heal in an environment where there’s no stress placed on those implants under function. And they go on and integrate,” Dr Rosenlicht says.
A single tooth does not get the same benefit from All-on-X implants as groups of teeth do, meaning that certain single-tooth, immediate placement procedures can be more difficult than multiple teeth because of the excessive lateral or occlusal loading, according to Dr Rosenlicht.
“A single-tooth implant placed and restored doesn’t have that cross arch stabilization. We have to make sure that the implant we’re choosing has the right design to maximize the stability,” he says. “Then we also want to make sure that we have components that we use on these immediate restorations that fit very well that stabilize the restoration that goes on to the implant. This is so we have no micromovement or no areas where bacteria can get involved in the junctions of the abutments on the implants. It also important to recognize that single implants may need to be provisionally loaded to avoid occlusal or lateral trauma during the integration period.”
Navigating Clinical Challenges
As with any dental procedure, immediate loading implants can present unique challenges for patients and practitioners. Standard implant procedures can put patients at potential risk for failed osseointegration, infection, or any number of problems ranging from discomfort to total implant failure. Added to the standard risks, immediate loaded implants come with their own set of risks.
With immediately loading implants, the risk of a tooth being used before it is ready to work can interrupt the fusion process, leading to failed osseointegration and a failed implant. There is also an added layer of complexity when factoring in the same-day extraction of the tooth in a single-tooth restoration, but the balm is experience, according to Dr Rosenlicht.
“You’re adding a little bit of complexity now to the surgery because the implant needs to be placed in an environment that’s healthy, with lots of bone. So the surgical extraction or removal of that tooth needs to be done carefully and by somebody who really does have experience in recognizing the nuances of what’s needed to be able to then place that implant after the extraction,” he says. “Taking that 1 step further, to do the immediate restoration at the same time, you need to be proficient in implant dentistry and oral surgery and [have an] understanding of all those issues that can cause failure, like if the patient isn’t chosen properly, the surgeries aren’t done properly, and so forth. I think that these types of procedures should be done by those clinicians [who] do have some degree of experience and have a comfort level in doing them.”
Another issue that clinicians may encounter is the bone itself. Because successful dental implants, including immediately loaded implants, are so dependent on the patient’s bone, habits, hygiene, etc, it is vital to understand who one is working with.
“We want to make sure we maximize the amount of bone that’s available, and in extraction sockets, oftentimes, the bone to the buccal in the maxilla is pretty thin, and the tissue also might be very thin, having a thin phenotype. Not only are we taking the teeth out and placing implants at the same time, but we also might be considering doing some concomitant bone and/or soft tissue grafting to be able to make this implant heal in such a way that we don’t have any future bone loss and where we minimize any potential for that to happen,” Dr Rosenlicht says.
Bone grafting can introduce a new set of problems for clinicians, and in those cases a clinician may need to delay implant loading. Although this may be a difficult conversation for the patient, assuring that the process is safer, more efficient, and less prone to issue will assuage concerns over the delay.
As with any dental procedure, contamination is an important consideration in the oral environment. Contamination is a key reason that Dr Rosenlicht and team do their best to avoid using cements in immediate load restorations.
“We realize how cements can be extremely contaminating to the environment and healing,” he says. “Most of our immediate implant restorations are done today with such sophistication that we can screw them down into the implant. And now we’re faced with implant position, so that the access hole for the screw that’s going to hold the crown onto that implant needs to be placed precisely.”
Boosting Precision for Best Results
With years of technological advancement, precision has become far more attainable than ever before. Tools such as surgical guides make implant placement that much more efficient, cutting time for the clinician and ensuring the patient is pleased with their implant results.
Dr Rosenlicht relies on digital navigation, a technology that has bolstered his immediate loading implant procedures.
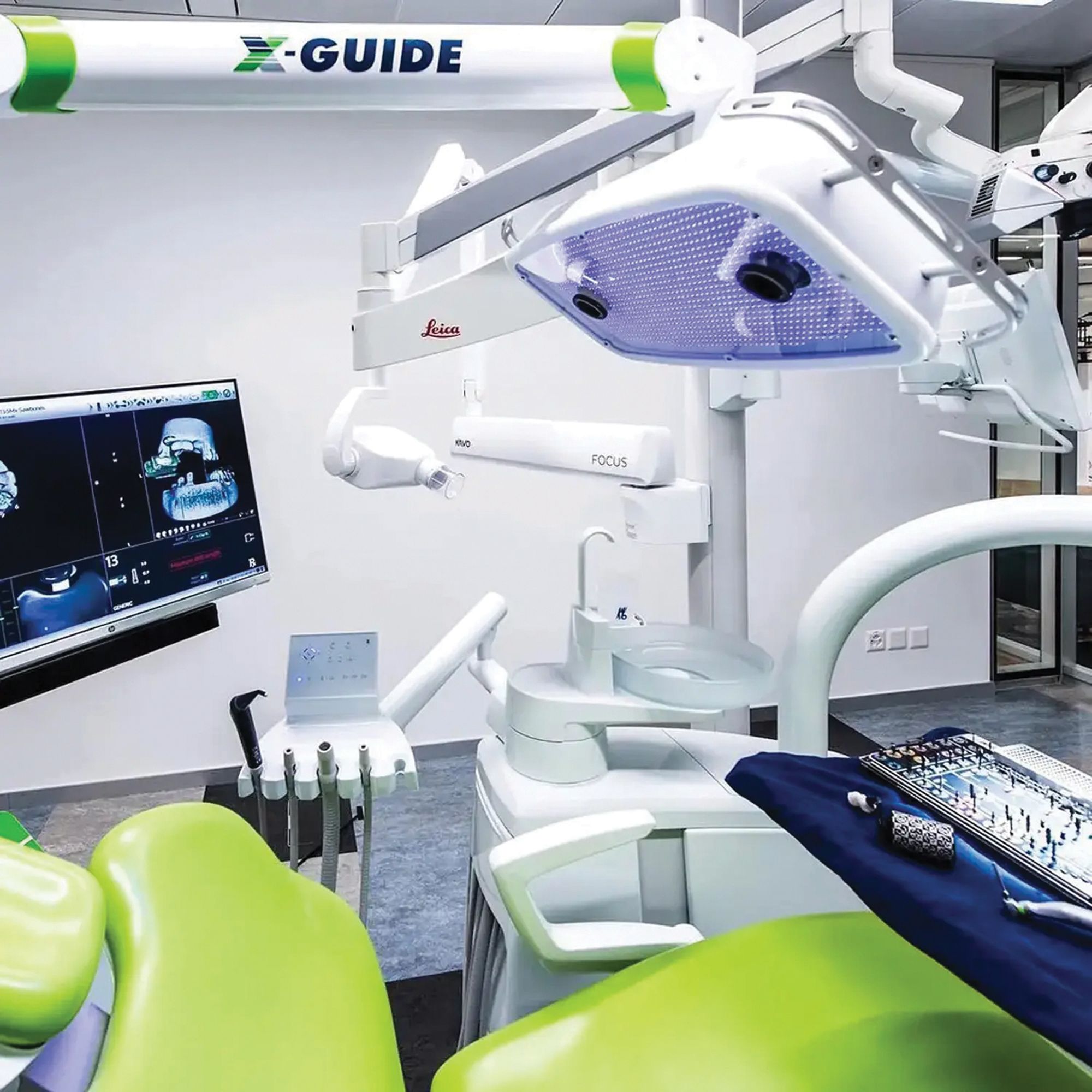
“We’re now doing these procedures with surgical guides, or with virtual navigation, such as the X-Guide® (X-Nav Technologies), which we’ve been using now for a while, where we can preplan our surgery with or without teeth present, and place them in the angle, the depth, and the position that we need to,” he says. “We can then construct that crown in advance that will screw down onto that implant in a cementless fashion that can be then removed or modified if necessary for the patient over time.”
X-Guide is a dental implant surgery solution with a variety of features to assist and guide clinicians. Its treatment planning system, 3D navigation, and live surgery guide are all designed to assist dental surgeons in obtaining the best possible outcomes for dental surgery. X-Guide is specifically designed for the same-day guided surgery that suits immediate loading implants the best.
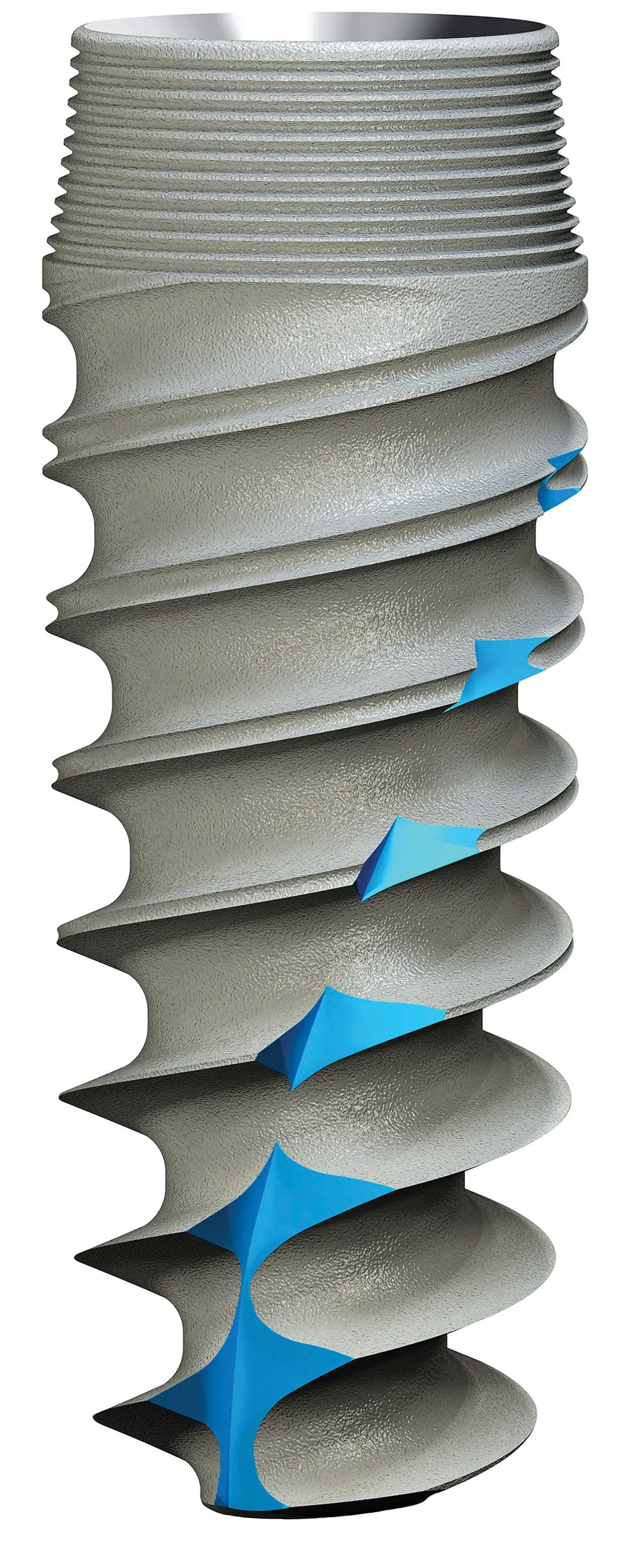
Dr Rosenlicht also says that the quality of the implant itself plays a very important role in the success of immediately loading implants. He finds Ditron Dental USA dental implants to be the best suited for this role, including the Ultimate Precision Implant (ULT™).
“One of the things that has evolved is the recognition of the stability that the implants need when they’re placed. Thread design is critically important. The design of the head of the implant also is becoming more critically important because we need to maintain bone levels at the crest of the ridge as best we can,” Dr Rosenlicht says. “The modifications of these newer generation implants, such as Ditron’s convergent head, and…reverse bone platform thread design, and the ability to have a precise abutment with the MolecuLock™ precision fit make Ditron Implants ideal for immediately placed implants and loaded implants.”
The Ultimate Implant from Ditron is a third-generation internal hex design that incorporates features such as the MolecuLock™ biomechanical implant-seal and the Reverse Concave Neck (RCN) with circular microgrooves to protect the soft tissue and crestal bone.
All About Stability
Immediate loading implants require 1 thing above all else and that’s stability. Without stability, patients with implants run the risk of peri-implantitis.
“Stability is key not only to the implant bone, but stability is key to the abutments and the crowns that go into these implants. Today so many implants are being placed in such a wide variety of patients, it is vital to recognize the health of the patient and the host response to that patient,” Dr Rosenlicht says.
“The most critical thing that we’re concerned about now is peri-implantitis because implants are not immune from developing infections in bone loss, just like teeth. With a lack of understanding of all these components that make for long-term success, you’re not going to have a great result,” Dr Rosenlicht adds. “You really need to understand and use those systems that offer the highest degree of success for the implants you’re placing in the restorations that you have planned.”
Immediate loading implants were the norm in the late 1970s and early 1980s, but clinicians and implantologists developed the more standard 2-system implant placement after numerous implant failures. These implant failures were caused primarily by a lack of understanding of the patient’s needs and the importance of stability. With this newfound understanding and a variety of tools in the implantologist’s arsenal, immediate loading dental implants have breached a new era in implant dentistry, according to Dr Rosenlicht.
“Now we’ve evolved again with the understanding of what causes failure. To be able to go back to what we originally did, it’s almost like we’ve come full circle, but with a high degree of success. This success is because of the computers, the planning, understanding the drilling techniques, and understanding compression of bone stability of the implants with a variety of different implant thread designs,” says the advisory board chairman for Ditron.
“With designs to minimize peri-implantitis and maximize bone healing around the head of those implants, we are even better now,” he says. “This is also considering the connections being so well adapted, and restorations easily and efficiently fabricated by the laboratory in advance, so that the time to get everything done is expeditiously done. These cases work out well.”
References
1. Cochran DL, Morton D, Weber HP. Consensus statements and recommended clinical procedures regarding loading protocols for endosseous dental implants. Int J Oral Maxillofac Implants. 2004;(suppl 19):109-113.
2. Morton D, Jaffin R, Weber HP. Immediate restoration and loading of dental implants: clinical considerations and protocols. Int J Oral Maxillofac Implants. 2004;(suppl 19):103-108.
3. Hof M, Tepper G, Semo B, Arnhart C, Watzek G, Pommer B. Patients’ perspectives on dental implant and bone graft surgery: questionnaire-based interview survey. Clin Oral Implants Res. 2014;25(1):42-45. doi:10.1111/clr.12061
4. Schulte W, Heimke G. Das Tübinger sofort-implant [The Tübinger immediate implant]. Quintessenz. 1976;27(6):17-23.
5. Singh M, Kumar L, Anwar M, Chand P. Immediate dental implant placement with immediate loading following extraction of natural teeth. Natl J Maxillofac Surg. 2015;6(2):252-255. doi:10.4103/0975-5950.183864
6. Fardal O, Linden GJ. Long-term outcomes for cross-arch stabilizing bridges in periodontal maintenance patients--a retrospective study. J Clin Periodontal. 2010;37(3):299-304.