The Realities of Open Architecture CAD/CAM
Learn how and why to build your custom CAD/CAM system with open architecture.


The Realities of Open Architecture CAD/CAM. Image courtesy of yalcinsonat/stock.adobe.com.

Building a custom CAD/CAM system in the dental practice presents a variety of unique opportunities for dental professionals. However, beginning that process requires an understanding of what open architecture CAD/CAM really is.
Open architecture describes CAD/CAM technology built using system code that is not proprietary and integrates with other components that use the same code, often from different manufacturers. In a closed system, the CAD/CAM system components use a private, proprietary code system managed by a single manufacturer, and they flow together automatically.
Some benefits of open architecture systems relate to the disadvantages of closed systems, which used to be the only option in CAD/CAM’s early days. John Flucke, DDS, technology editor for Dental Products Report®, describes the concept behind open architecture and interchangeable parts as a significant improvement over the closed system. “The dearth of CAD/CAM system options in the early days locked a dental practice into a closed system with 1 manufacturer. That wasn’t a problem unless the clinician didn’t like it or was unhappy with the performance of a component in the system,” Dr Flucke explains. Although the companies always responded if clinicians weren’t happy, he says closed systems were a tough deal for the dental practices in these cases.
Furthermore, buying options were closed systems through exclusive partnerships with large distributors. If a dental practice didn’t have a strong relationship with the distributor that sold the closed system, it was harder for the practice stakeholder to invest the 6 figures required.
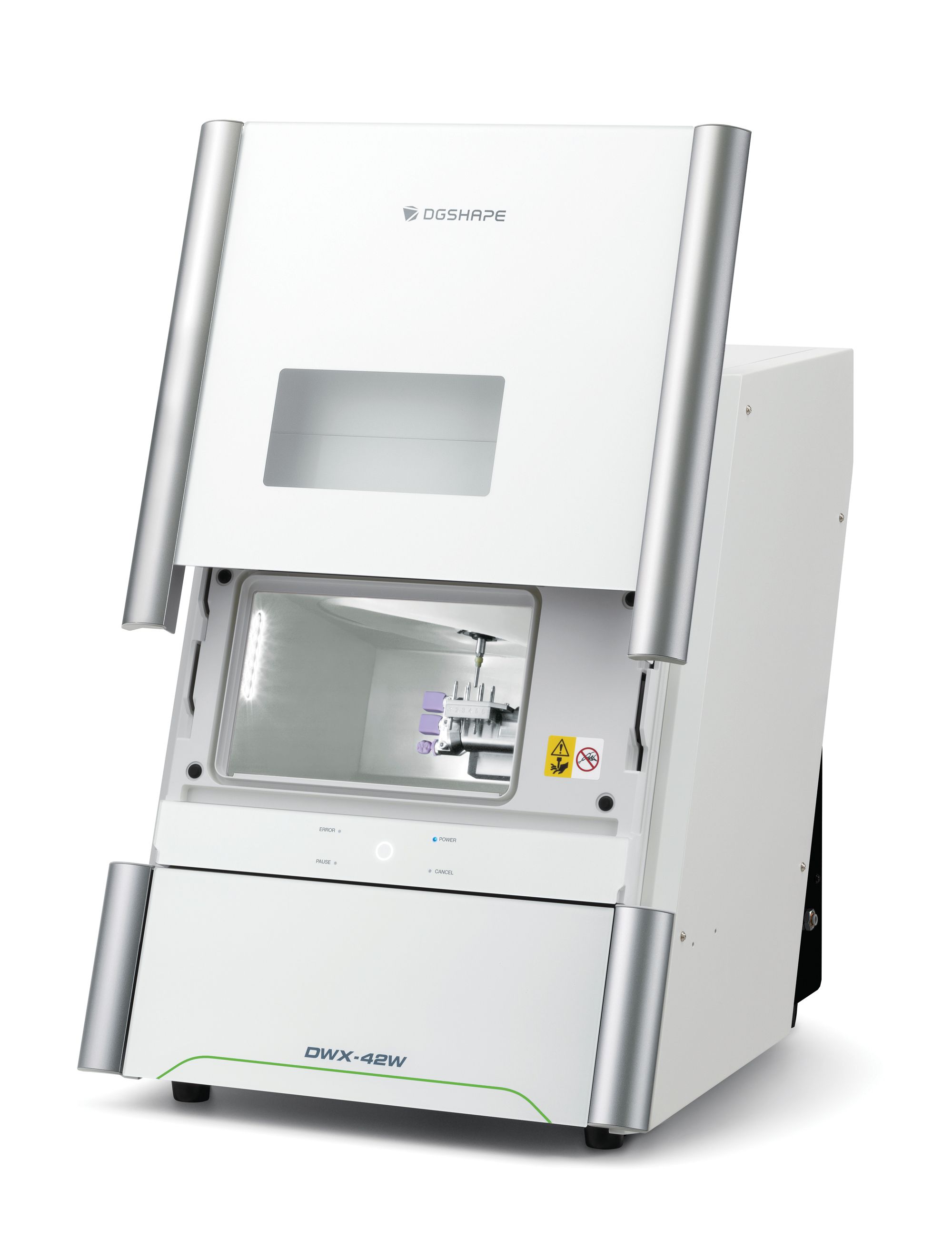
With open architecture systems, practices can combine companies within the workflow. For example, Dr Flucke says he scans with iTero, designs with exocad design software, and mills with Roland DGA’s DGSHAPE DWX-42W. “The other great part is that if a company comes out with this great intraoral scanner that has 100 different things and all [are] better than what I have, I can buy the new one, and it will interface with these pieces I already have in place. So that’s huge,” Dr Flucke says.
As a result of open architecture, dentists can mix and match equipment and software to get jobs done. Marty Jablow, DMD, agrees that open architecture means freedom. Dr Jablow is chief development officer for Cellerant Consulting Group, a specialized boutique consulting firm for dental companies, and owner of The Dentists of Woodbridge in Woodbridge, New Jersey. “You can do exactly what fits your needs best. However, the best is not a one-size-fits-all situation,” Dr Jablow says.
Lisa Aguirre, marketing manager of dental solutions for Roland DGA, also thinks the versatility of open architecture systems increases accessibility for chairside restorative dentistry. For example, the DGSHAPE DWX-42W chairside milling solution allows a practice to choose their scanner (either one they have or one they need to buy) and their design software. Also, open architecture systems mean that the process for sending work to the lab can be the same for the in-house workflow. “With the old, closed turnkey system, you are limited to components within the same system,” Aguirre says.


The DGSHAPE DWX-42W from Roland DGA allows the dental practices and labs that use it to adopt and combine different components in digital workflows. This provides a unique flexibility for clinicians and technicians that they wouldn’t be able to take advantage of with a closed system.
Open architecture also allows teams to switch out a component, such as a scanner, if the practice wants to try a different one. The system will enable them to do so without compromising the other parts of the workflow. “With our system, you can use both of them,” Aguirre explains. “You can always add technology, and nothing you’ve already invested in becomes obsolete unless you want to kick it out.”
Aguirre says open architecture lets clinicians choose their material based on the patient’s esthetic and functional needs. Closed system users are limited to contracted materials for that system. “If they want to add materials as they become available, typically there are costly upgrade fees or additional packages that need to be purchased,” Aguirre says about dental practices with closed systems.
Rune Fisker, senior vice president of product strategy and product management for 3Shape, says that open architecture allows you to choose the best of everything. Having the best of all significant components enables you to have a more competitive solution. Additionally, open architecture manufacturers are continually optimizing connectivity between components. “All this is coming together,” Fisker says. “Much progress has been made connecting individual dots, so it becomes a smooth workflow where you don’t have to buy a system [for] $140,000. Open architecture makes it combined, much cheaper, and you can select the best technologies from different manufacturers and still have an easy-to-use workflow.”
What to Consider When Building Open Architecture CAD/CAM Systems
Regarding the open architecture building process, Aguirre says dental practices should look for an option that fits their budget. Depending on which components dental practice stakeholders choose, the cost of a complete system built with open architecture can be as low as $60,000, far less than the $100,000 cost of many closed system workflows.
After the budget consideration, Aguirre says the most important thing is to build something that suits the needs of your dental practice. Dental practices often realize they need something else after they acquire a new system. Open architecture systems allow the practice to add something new and mix and match. “Versatility is important because our industry changes frequently,” Aguirre says.
Fisker says the certainty about what indications you will address with the system will also drive purchasing decisions. Some practices may want to do everything with CAD/CAM, which is excellent according to Fisker. In that case, he recommends making a prioritized list of workflows. For example, what indications does the practice want to address in-house? Does the dental practice wish to design restorations themselves or hire a service? Do they want to mill single zirconia restorations or 3D-printed complete dentures? These considerations will affect the decision. “Then think carefully about who uses it in the dental practice. Will you have an in-house technician, or do you want your assistant to take care of it?” Fisker says. “If it’s an in-house technician, then you can be a little more adventurous on how connected the workflow is and how smoothly they work together. But if it’s the assistant, you might need a focus on easy workflows and smooth integrations.”


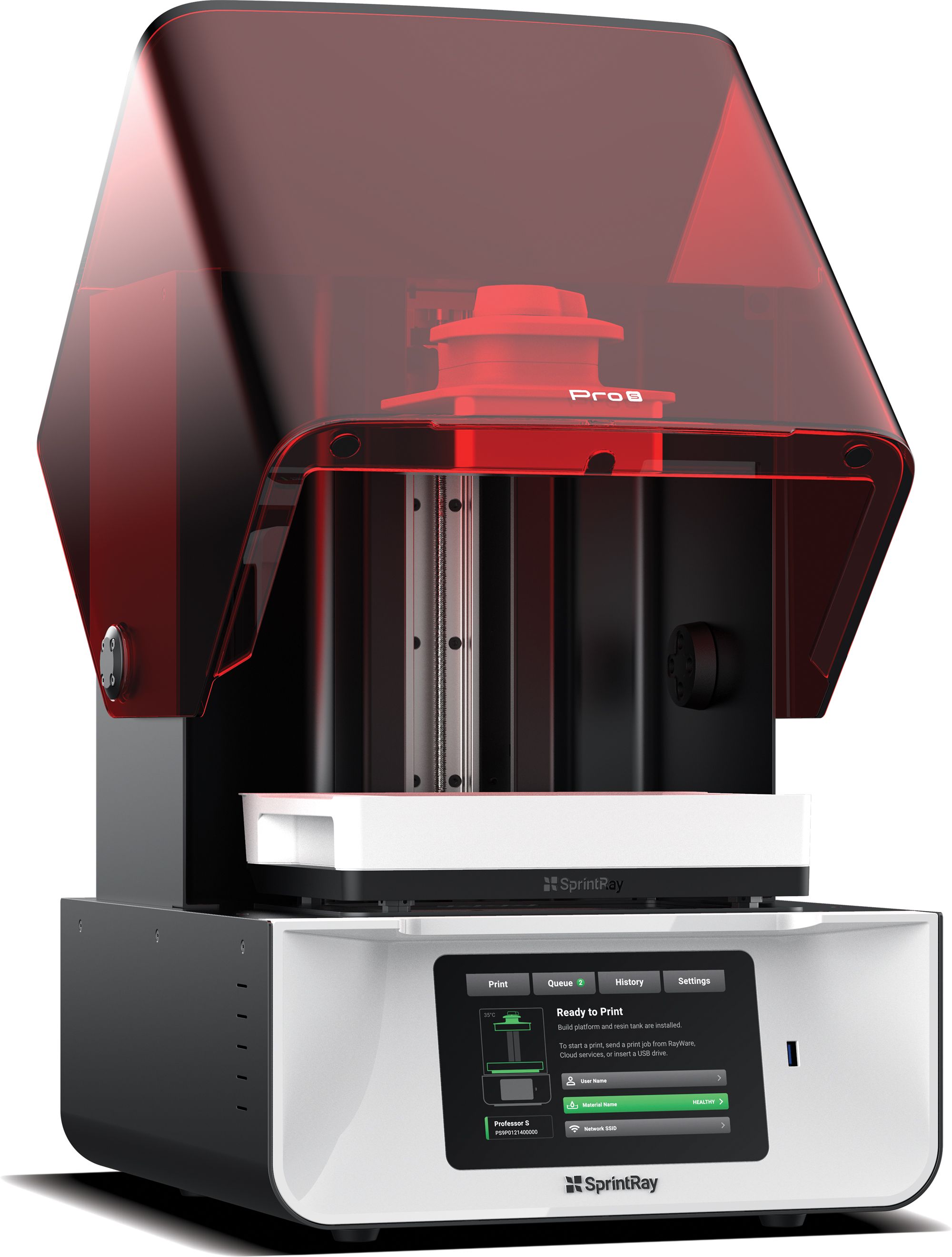
SprintRay 3D printers, such as the Pro S shown above, use open cloud software called SprintRay Cloud Design. This makes it easy for clinicians at any skill level to have a more structured and guided workflow when 3D printing a variety of dental apparatuses.
Streamlining workflows is a significant part of 3Shape’s product development. 3Shape released the newest version of their dental laboratory CAD software, Dental System 2022, in early October to provide intuitive workflows for many indications. The software improves communication between labs and dentists and streamlines digital integrations. These same connectivity improvements are a developmental focus for all 3Shape product lines. “We can build something that is not just open architecture but [is] also connecting and creating smooth, integrated workflows,” Fisker says.
As a lecturer and author on dental technology, Dr Jablow teaches dental practices how to incorporate the latest dental technology in their offices to benefit patient care and comfort. He agrees that connectivity can be an issue. He cautions practices to remember that the freedom to mix and match has a cost. Troubleshooting can be more challenging if it is unclear which technology has a problem in the workflow. Open architecture often means multiple vendors pointing at another vendor when there is a glitch.
“The software will point to the hardware, and the hardware will point to the software,” Dr Jablow explains, adding that closed systems have nothing to point at but themselves. “You have to understand that you may run into roadblocks here or there that you’ll have to navigate around, because the open system allows different companies to shift the blame.”
Learn From Clinicians Who Have Used Open Architecture
A common mistake that practices make when purchasing open architecture systems is having the wrong expectations beyond initial implementation. Dr Jablow explains that building one system into another and adding new technology piecemeal means learning every procedure individually. As a result, there may be several trainings. “You might have to learn software, the integration process, and the different parts of the system, then master them and put [them] all together,” Dr Jablow says. “You also must understand what you are getting with each piece, [such as] warranty or long-term reliability issues. So all those things come into play.”
For example, most systems have updates, and Dr Jablow thinks some dental practices don’t consider the frequency of software updates and the associated costs. With several manufacturers involved, there could also be multiple updates and fees. Updates to one part of the workflow could cause hiccups with another part until it gets upgraded. “Say there’s a feature you want in your design software, and you go get it. But now you have to update the firmware in the mill or printer to work with the software. If you fall behind, that could be a problem,” Dr Jablow says.
Dr Jablow says that calculating a 5-year average cost for updates in addition to the purchase price can help a practice prepare and adjust its expectations before building. Also, learning about fees associated with software or hardware and how long the technology will get support from the sales representative are essential pieces of the puzzle. Moreover, Dr Jablow says hardware is forever until it isn’t. “If you don’t pay the annual maintenance,” he says, “then it becomes [a] doorstop.”
Aguirre cautions practices against unrealistic expectations, which impede implementation success. If the system does not meet expectations, the team may give up on it. Instead, she recommends involving the team early and getting them excited about working with the open architecture system.
She says Dr Flucke did a great job with this in his practice. “He took one piece of the puzzle at a time. His staff was excited to do this for their patients and learn about it,” Aguirre says, adding that they waited almost a month after the implementation of the Roland DGSHAPE chairside milling solution before delivering a same-day restoration. “They were very selective about the patient they chose. They said, ‘Hey, we have this new technology, and we want to [use] it the same day. Are you game?’ The patient was. So it’s about knowing your patients and setting realistic expectations.”
Aguirre cautions against thinking you will “build Rome in a day.” Instead, she encourages practice leadership to respect the inherent learning curve. For example, clinicians may begin by scanning and designing one day and having the patient return for delivery on another day. Then, once the practice has a system, they can provide same-day delivery.
In addition, all dental staff should learn the benefits of CAD/CAM for the patient. For example, they should be able to explain to patients how same-day dentistry eliminates the need for temporary restorations or how digital x-rays have less radiation and are more comfortable. She says that positioning the workflow as an investment in the patient experience and improving patient care are excellent ways to leverage the benefits of an open architecture system.
Fisker agrees that ignoring the staff’s level of experience with technology and their desire to have experience with technology is a common misstep with open architecture CAD/CAM systems. The freedom a dental practice can realize with an open architecture system also has different graduations of user-managed complexity. For example, dental practices that buy a SprintRay printer will have more guided workflows available than practices that buy a less expensive printer.
A similar example would be individual preferences regarding personal technology. Some people choose Apple because the iOS system doesn’t require networking expertise when adding another Apple device. In contrast, some personal computer users enjoy building a system from the ground up to create an individualized experience. Getting the various components to talk to each other is part of the fun. Fisker says it is essential to determine where the staff who use the CAD/CAM system most frequently fall on the spectrum between intuitive connectivity and total freedom. “Are you able to build the [personal computer] yourself? Or do you need an Apple [system] that is super smooth?” Fisher explains.
As these connectivity issues become less of a problem through development, Fisker sees a future where the preferred system for CAD/CAM is open architecture. Fifteen years ago, lab systems were closed systems; today, the lab world is completely open architecture, he says. He sees similar changes happening in the printer market as well. “I am not in doubt that open [architecture] will prevail,” Fisker says of CAD/CAM systems. “But of course, the open systems need to be good enough in terms of ease of use and efficiency.”

















