How to know if you’re using the right curing light
Not only do you need to understand how the various restorative materials handle and how they work for different procedures, it’s also key to stay on top of what curing lights work best with what material and exactly what it takes to ensure you get the best results.
Not only do you need to understand how the various restorative materials handle and how they work for different procedures, it’s also key to stay on top of what curing lights work best with what material and exactly what it takes to ensure you get the best results.
3M ESPE scientist Joe Oxman said it’s important to realize your materials and your curing light need to work together properly to make sure your patients get the best possible care.
“If you don’t cure it properly you can end up with reduced properties, you can end up with more staining, more extractables, so adequate curing is really the key to success,” said Oxman, who has worked at 3M ESPE for three decades.
“Traditionally there had been two limitations with materials: No. 1 it was challenging to get sufficient curing from top to bottom; so to try and cure something from top to bottom 4 mm was challenging. But the bigger issue is that when these materials undergo their curing or hardening process is they tend to shrink.'



"The problem that you run into is if the materials exhibit too much shrinkage then the more material you place the more potential issues that you could have in terms of the material not anchoring well or adhering well to all the walls of the tooth structure.”
Because of this, Oxman said it takes a lot of research before you understand how materials and curing lights work together. Companies also need to conduct plenty of tests before launching new dental restoratives and curing lights. Numerous studies need to be conducted before researchers determine that products like bulk fill materials will deliver strong restorations.
“What we’ve tried to do is develop this new



material that can not only be cured at a depth of 4 mm from top to bottom, but also it has low shrinkage and shrinkage stress,” Oxman said, talking about how 3M™ ESPE ™ ’s Filtek™ Bulk Fill Flowable Restorative came about. “But at the same time we’re trying not to compromise mechanical properties and things like abrasion resistance. That would be a good example of how we try to combine materials along with light curing to provide something that can ultimately save time.”
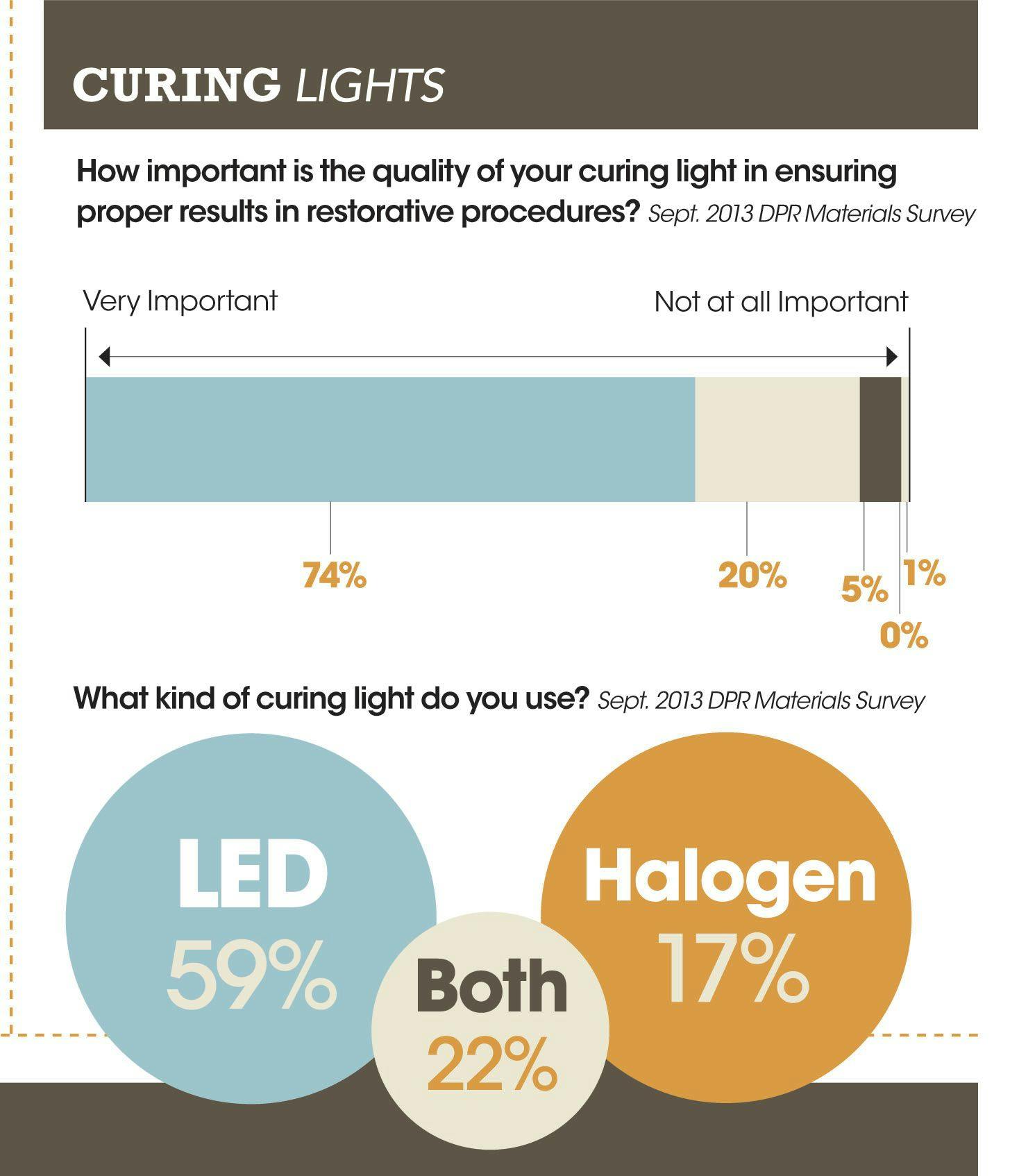
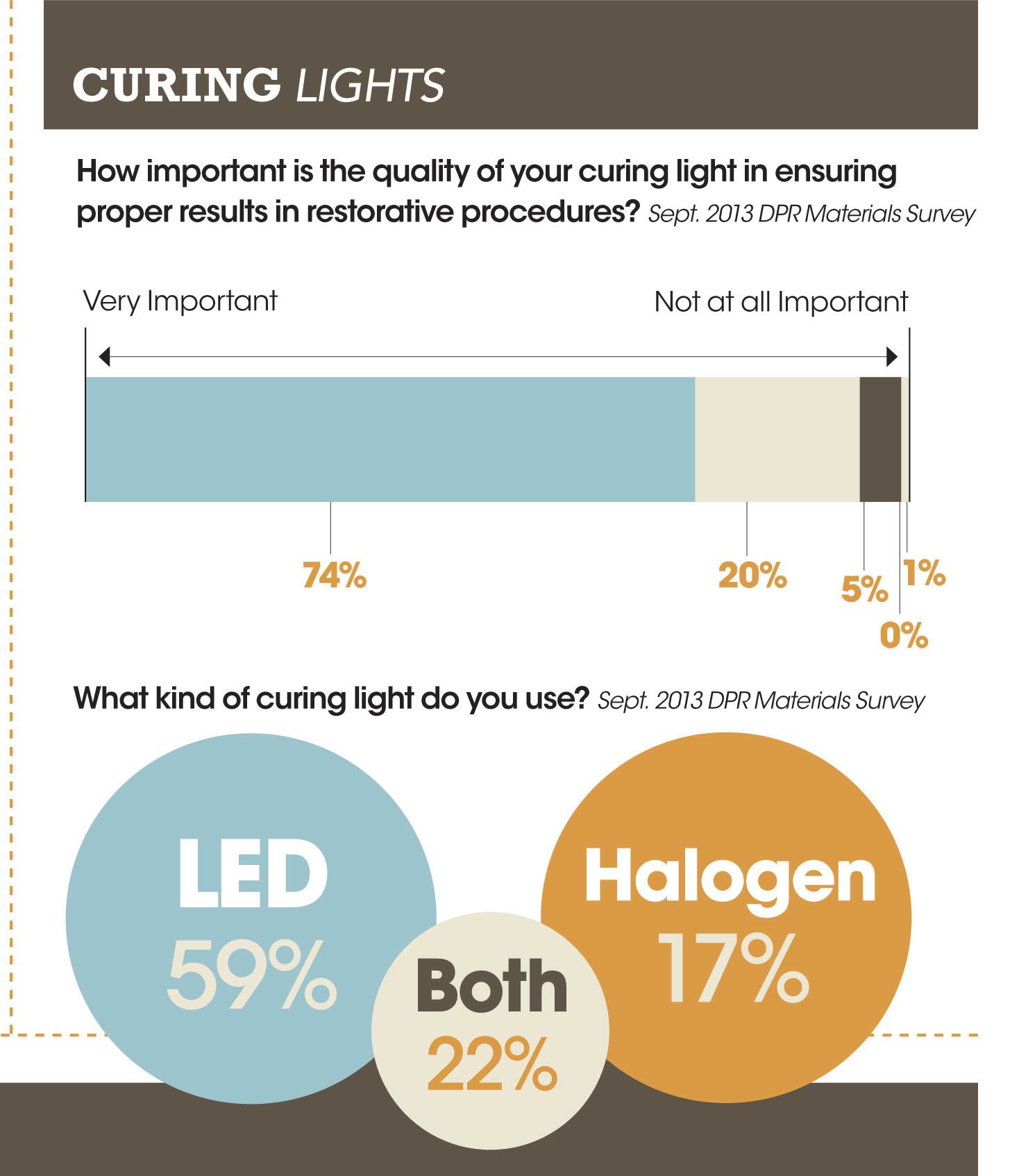
A decade ago halogen lights were quite popular in the industry, but the shift to LED lights is reflected by DPR ’s latest survey. Almost six in 10 respondents (59%) now use an LED curing light, while 17% use a halogen light (22% use a combination of both types in their practice).
“LEDs provide the benefits of being energy efficient. They don’t need to be replaced, they have high output and they provide the ability to use a battery-operated source,” Oxman said.
“So there’s going to be some continued advancements in the lights, but the lights by themselves don’t serve a useful purpose without the materials, and the material by itself isn’t useful without the lights. It’s the combination of the two-it’s the system that’s critical to the end result.”



Dr. Daniel Ward said it is important to understand how your curing light works with a variety of today’s materials.
As is always the case, following manufacturer instructions is a key step that should not be overlooked. He added, however, that information is not always easily accessible when you’re working with numerous products and are unclear of how exactly each one will interact with your curing light.
“It is not always easy to ascertain the photoinitiators employed for a particular brand and/or shade of composite,” Dr. Ward said. “It is certainly not printed on the side of the composite syringe nor prominently listed on the directions for use (DFU).’
“Some composite materials may use different photoinitiators within the same brand of materials. The most common used photoinitiator is camphoroquinone, which is yellow in color.
“Companies often use dif ferent initiators in their translucent incisal shades to allow for a more clear-blue/gray color,” added Dr. Ward, who has lectured at the Post-Graduate Programs in Esthetic Dentistry at the University of Minnesota, SUNY Buffalo, UMKC ,

and the University of Florida and served as chief examiner.
“Recently new photoinitiators have been introduced that are more sensitive to light output, allowing for a deeper depth of cure. It is better to use a curing light that emits multiple wavelengths of light; 470 nm blue light, which cures camphoroquinone, and 390-435nm purple light, which cures many of the other photoinitiators used. Light output is very important. The latest generation of LED lights have incredible energy output to ensure that the material is adequately cured for optimal performance.”
Oxman warns, however, that some materials require a minimal amount of curing time even when high intensity lights are used. He suggests clinicians make sure the cure is complete before moving on to the next step.
“Really the take-home message now from a number of researchers is that the exposure time is more important than the intensity. I’m not saying the intensity isn’t important, but if you really step back the studies are saying you really need to have a certain amount of light exposure,” Oxman said.
“Again it’s going to vary depending on the shade of the material and the optical properties. The message is that there is some limitation with the chemistry. You need to cure it effectively at the top and you need to cure it effectively at the bottom and that there’s some kind of minimum light exposure.”
Dr. John Comisi suggests dentists shop around when considering a curing light purchase as today’s options offer up a wide range of features.
“First they need to know what the energy output of the light happens to be, and how the energy is maintained as the light is further and further from the deepest aspect of the preparation,” he said.
“Second will it cure all materials? Is the wavelength of the light output going to do the job? Third can the light’s battery be replaced, and if so is it at a reasonable cost? All batteries eventually will need to be replaced since they will lose the ability to recharge after a period of time. If the cost is high, then that becomes a consideration in purchasing the device. If the battery cannot be replaced, then the entire device will need to be discarded and a new one purchased. These costs are important to keep in mind.”
Dr. Tysowsky notes that curing lights have become such a common staple in practices that clinicians pretty much take them for granted. But again, it is critical to the restoration’s success that the curing process be sufficiently completed.
“As per the survey conducted by ADA 2005-2006, approximately 116 million restorations are placed in the U.S. each year,” Dr. Tysowsky said. “Dental composites are a major part of dental practices for over a decade. It has been well documented in the literature that the adequate polymerization of resin composites not only determines their physical and mechanical properties, but ultimately the clinical success of a restoration.’
“On the other hand, inadequate polymerization results in inferior physio-mechanical properties such as poor resistance to wear, color instability, increased rates of water absorption, increased solubility-all of which can result in compromised clinical performance.”
Proper curing is needed for more than just resin composites; it’s also needed for curing lights to achieve required clinical outcomes with resin cements, adhesives, provisional, and core build up materials. Therefore, the curing light is an important component of a dental practice and clinicians should consider attributes like power output, curing modes, wavelength range, depth of cure, exposure time, and ease of use before making a decision.

“Contemporary resin composites are light cured via radical polymerization,” Dr. Tysowsky said. “The energy from curing lights is absorbed by molecules called photoinitiators, which enable the formation of radicals to initiate the complete cure of composites. Dental composites constitute individual or a mixture of photoinitiators like camphorquinone, Lucirin, TPO and Ivocerin with a wide range of absorption spectra. Curing light spectrum outside photoinitiators absorption spectrum doesn’t cure materials completely and results in inadequate curing.
“Secondly, with the significant increase in the use of ceramic or zirconia restorations, depending upon clinical situations, clinicians use light cure or dual cure resin cements,” he adds. “Light energy attenuates when passed through a medium like tooth or ceramic restoration, and percentage of light attenuation depends on translucency and thickness of ceramic material. According to Total Energy Concept, 12-16 Kilojoules of energy is required to cure resin materials.
“Therefore, while selecting a curing light clinicians should understand his/ her needs depending upon the type of materials used in the dental practice and should select a curing light with a broad wavelength spectrum, high power output, continuous curing, ergonomic design, a contact free battery and easy maintenance.”
The science behind all of today’s dental materials and curing lights may be difficult to stay on top of, but Oxman does offer up some advice to help.
“There are a variety of very simple things that clinicians can do to succeed, or to increase their success rate with light curing,” Oxman said. “It’s really critical that the light be placed directly above the material you are curing. If you’re off by a millimeter or two, then your curing can be off.”
Just don’t go too close.
“You should hold the light as close to what you are trying to cure as possible without actually touching it,” he said. “If you touch the material you might stick to the light, contaminate the light or you may impact the anatomy.”
Oxman’s other advice includes making sure you have sufficient cure time and that you maintain the device properly. He suggests that from time to time clinicians calibrate the light source just to make sure it is providing a constant output. Also, users need to periodically clean the light guide because the end of the light guide can get contaminated.
According to our survey, dentists are clearly aware of the importance of curing lights. When we asked how important the quality of your curing light is in ensuring proper results in restorative procedures - on a scale of 5 for very important and 1 for not important at all - 74% checked 5 (most important) and 20% checked 4 (next most important).










