Changing the Script: Efforts to Curtail Overprescribing in Dental Practices
As the opioid epidemic rages on, it’s time the profession recognizes the role it has played in the crisis.


©Alexander / stock.adobe.com

There is perhaps no health crisis in the past 2 decades that has come close to the current opioid epidemic. It wasn’t until the past decade that patients and prescribers began to truly understand the dangers of opioids. but the damage has been done. As opioid-induced deaths continue to climb, it is critical for the dental community to understand its role in this crisis and develop prescribing best practices.
The Beginning
The fact that opioids are highly addictive substances is widely acknowledged in medicine and among the general public. However, that was not always the case. Although the phrase “opioid epidemic” would not be coined until later, the crisis itself started in the 1980s and 1990s, during which a fundamental shift occurred in the way pain was treated by health care professionals.1
In 1990, Annals of Internal Medicine published an editorial written by the president of the American Pain Society that criticized the seeming lack of improvement in pain management over the past 20 years.1 The argument was that education and guidelines were not working—a failure attributed to patients not being up-front about their pain with health care providers and a general reluctance among clinicians toward prescribing opioids.1
The widely accepted wisdom was that “therapeutic use of opiate analgesics rarely results in addiction,” however, this was found to be based on a single published study with few details on how the study was completed.1
The following year, the American Pain Society introduced its quality and assurance standards for the relief of acute pain and cancer pain. Recommendations included the following1:
- Chart and display pain and relief.
- A simple and valid measure of pain should be selected by each unit.
- Each clinical unit should identify values for pain-intensity rating and pain-relief rating that will elicit a review of the current pain therapy.
The last recommendation is likely to have led to the use of pain treatment algorithms that later proved highly problematic, especially in hindsight.1
Although this was the beginning of more aggressive treatment of pain, the acceptance of pain as the fifth vital sign began even earlier, says Mark Donaldson, PharmD, BSP, ACPR, FASHP, FACHE, associate principal at Vizient, Inc, a health care improvement company based in Irving, Texas.
“If you go back to the late 1970s, beginning 1980s, there was a focus from the Institute of Medicine (IOM) that pain should be considered the fifth vital sign,” Dr Donaldson says. “Patients, as well as providers and insurance companies, really recognized that we have lots of great medications out there and interventions. And so there should be a better attempt at managing pain because it is truly crippling not only to the patient but to their loved ones, [and to the patient’s] ability to be a productive member of society.”
In 2000, then-president of the Joint Commission on Accreditation of Healthcare Organizations, Dennis O’Leary, MD, announced the standards for health care organizations to improve pain management. Dr O’Leary emphasized the need for these standards due to confusion over who was responsible for pain control, a general lack of knowledge about pain management, and misconceptions about drug tolerance and addiction. His outlook was consistent with similar positions expressed by the IOM (now the National Academy of the Sciences), American Pain Society, and US Veterans Health Administration. Although these standards were lauded by pain experts, there was concern they would lead to an overreliance on opioids. Regardless, the use of opioids continued to increase into the early 2000s.1
“Pharma companies certainly do shoulder a lot of this blame,” says Dr Donaldson. “They picked up on the IOM report that pain is a fifth vital sign and that we need to start treating more aggressively, primarily with narcotics. They started to put out a little bit of misinformation that really sort of underplayed the danger associated with getting patients on narcotics.”
“There was a general misperception that perhaps these drugs were not addictive,” says Rebekah Lucier Pryles, DMD, an endodontist and co-owner at Upper Valley Endodontics, and an instructor at Harvard University School of Dental Medicine and Tufts University School of Dental Medicine. “We’ve learned that that’s obviously not the case. And we’ve also learned a lot more about how to manage both acute and chronic pain. Quite honestly, some of the push of treating pain as a fifth vital sign came from the pharma companies and the fact that doctors needed to address pain.”
In the 1990s and early 2000s, the pendulum began to swing the wrong direction, Dr Donaldson says, adding that this was when a lot of opioids were also prescribed for postoperative dental pain.
“It was almost 2 decades in the making,” Dr Donaldson says. “We’ve had problems since the early 1980s, when overprescribing first started. And the overprescribing actually coincided with some marketing strategies by pharmaceutical companies, most notably at the time was Purdue [Pharma], who makes OxyContin. You have this issue where the Institute of Medicine [was] pushing prescribers to recognize and treat pain more effectively. You [had] pharma companies coming out saying, ‘Ours is the best. Ours does not cause addiction.’ That was one of the big misnomers but was part of the original OxyContin and oxycodone marketing. So we ended up getting a lot of people, unfortunately, hooked on narcotics.”
This was the start of what we now recognize as an epidemic; nearly 841,000 Americans died of a drug overdose between 1999 and 2019. In 2019 alone, 70,630 drug overdoses occurred in the United States, 70.6% of which were opioid-related. Opioids, and more specifically, synthetic opioids, are the main drivers of drug overdose deaths.2
In a 12-month period ending April 2021, more than 100,000 Americans died of an overdose, a 30% increase from the previous year. This marks the first time the US has exceeded 100,000 deaths per year, which is more than motor vehicle accidents and gun fatalities combined.3
Dentistry’s Role
These stark numbers serve as a reminder why health care professionals, including dentists, should exhibit caution when prescribing opioids—if opioids are to be used at all. Many individuals addicted to synthetic opioids likely became addicted after being given prescription opioids by medical providers.3
Between 2011 and 2015, dentists were responsible for 1 in 10 opioid prescriptions in the US, with 29% of prescribed opioids exceeding the recommended morphine equivalents for appropriate management of acute pain.4 Approximately half (53%) of these prescriptions exceeded the recommended days’ supply, and between 1 in 4 and 1 in 2 opioids prescribed to adult dental patients are overprescribed.4
The attitude in health care was that not giving patients strong pain medication meant clinicians were neglecting their patients’ care, says Brooke Blicher, DMD, an endodontist and co-owner at Upper Valley Endodontics with Dr Pryles, and an instructor at Harvard University School of Dental Medicine and Tufts University School of Dental Medicine.
“If you’re not giving pain medication, you’re a terrible provider, [and] you’re ignoring your patient. Dentistry definitely got wrapped up in that. I think this isn’t just dentistry, but you form a lot of your habits when you train. [So, people in the ’80s and ’90s] were trained to give opioids, and that’s what we were doing. [We] didn’t know any better [then],” Dr Blicher explains.
“I think that dentists have in the past predominantly prescribed opioids for moderate to severe pain in a lot of their patients, probably more so than nonopioid drugs,” says Arthur Jeske, DMD, PhD, professor and associate dean for strategic planning and continuing dental education at The University of Texas Health Science Center at Houston School of Dentistry, editor in chief of Mosby’s Dental Drug Reference, and editor of Contemporary Dental Pharmacology. “But the quantities that they prescribe in no way exceed those prescribed by physicians. One of the reasons for their previous reliance on opioids has been the fact that opioids are controlled substances and are perceived to be superior to other pain control entities because they are subject to [US Drug Enforcement Administration] control.”
It is true that dentists are not solely responsible for the previous attitudes in medicine surrounding opioid use. A 2017 study from National Public Radio found that dentists ranked fourth in 2012 in opioid prescribing rates when compared with their medical colleagues.5 Although, historically, dentists and oral surgeons were robust utilizers of opioids in pain management, Dr Pryles says that has changed over the past few years as new information and best practices have become available.
“Dentists have significantly curbed their prescriptions of opioids in the past 5 years thanks to the availability of new information that’s out there,” Dr Pryles says. “I think the large numbers of prescriptions that were available, there were twofold reasons for them: First, there was a push from big pharma to get these drugs into patients’ hands, and the misperception that perhaps they were not addictive [was] being spread as well. I also think that there was a lack of good resources and good research on pain management. I think we swung from a culture in medicine and dentistry of patients being told to suck it up—that pain was normal—to the complete opposite end of the spectrum, where we as clinicians had to get rid of all of patients’ pain,” she says.
More recent data show that opioid prescriptions are trending downward. A study published in August 2021 in the Journal of the American Dental Association found consistent decreases in opioid prescription rates in dentistry during the study period.6 The results showed a decrease in the percentage of patients receiving an opioid in a given year, declining from 2.7% in 2012 to 1.6% in 2019 among children (aged 0-20 years) and from 28.6% to 12.2%, respectively, among adults (aged 21-64 years). Although this pattern is encouraging, investigators noted these results still show that the overall rate is still too high and that prescriptions are being written unnecessarily.6
“I think the concern that dentists have is that patients may be undertreated for pain,” says Mea A. Weinberg, DMD, MS, a clinical professor of periodontology and implant dentistry at the New York University School of Dentistry. “They don’t want them to go home in pain. They think they need to do the top of the line so that the patients will not feel anything.”
Over time, dental opioid prescribing has decreased by approximately 20%.7 Although this decreased trend is certainly a positive, it comes too late for so many. It’s hard to reverse course with such addictive substances, Dr Donaldson says.
“Over the last 10 years with the recognition of the opioid epidemic, we’ve tried to reverse the Queen Mary, but that’s been a significant challenge,” he says. “Of course, narcotics are very addictive, certainly in [particular] patients. One in 16 patients who have a single dose of an opioid will become an addict...and you just don’t know who that 1-in-16 person could be.”
An individual can be introduced to opioids in a dental setting at a young age, which is mainly attributed to third-molar removal. A 2018 study suggested that opioid-naïve patients who receive an opioid prescription from a dental clinician may be at risk for persistent opioid use and abuse.8
“Young adults usually get their wisdom teeth removed around the age of 17 to 18 [years],” says Walter Tatch, DDS, FACOMS, an oral surgeon at NorthShore Center for Oral & Facial Surgery and Implantology near Chicago, Illinois. “It is possible that they may have their first experiences with opioids at that time. We have clearly shown in our practice over a number of years that it is possible to use alternatives to heavy opioids to adequately control pain and avoid abuse potential.”
Impact of COVID-19
COVID-19 has exacerbated many systemic health care issues across the board—including the use of opioids and other addictive substances. COVID-19 pandemic–related stresses have triggered an increased use of opioids, alcohol, and cannabinoids.9 In addition, data show at least a 15% increase in stress-associated dental or oral health complaints—including daytime clenching and nighttime grinding—versus pre-pandemic times.9
“It’s hard to think that [COVID-19] doesn’t have an impact on [all walks] of what used to be our normal lives,” Dr Donaldson says. “Certainly, during the early days of the [pandemic], [when] people were encouraged to social distance, mask up, stay at home, you saw a significant drop in patients going to the dentist. Unless it was for an emergency procedure, patients have preferred to stay out of hospitals, stay out of dental offices, stay away from everybody. I still think that [although] we have historically always been encouraged to visit our dentist every 6 months for [a] routine hygiene checkup, because of COVID-19, people put a lot of that off.
“Now that they may be returning to the dental office because they have been less proactive in their oral health care, they’re coming in with worse situations, maybe more painful situations,” he continues. “Through preventative measures caught early on, they might not have proceeded to the point [at] which they now require significant pain management to get on top of their issues.”
This, Dr Donaldson says, is putting undue pressure on dental prescribers, who are being told by their patients that acetaminophen and ibuprofen are no longer working.
Although Dr Tatch never closed his practice during the pandemic, he understands that COVID-19 has resulted in consequences for dental patients.
“I do oral maxillofacial surgery, so we never closed our practice. We went from seeing regularly scheduled patients to emergency patients—patients with severe infections, facial trauma, and things like that,” he says. “But [not] having exposure to dental care, that certainly impacts dental health if patients are not [being seen] in general dentist offices for their routine care for the cleanings. A lot of patients have significantly increased cases of temporomandibular joint problems because of stress, impaired function, and that goes along with not being able to be seen in dental practices for their routine appointments.”
COVID-19 not only forced practices to close for several weeks during 2020, keeping patients from much-needed care, but it has also underlined the fractures already present in the health care system. Systemic disparities in access to treatment, gaps in insurance coverage, and economic instability were at the root of the opioid epidemic before the COVID-19 pandemic took hold.9
Early data suggest that COVID-19 and efforts to mitigate the spread of the SARS-CoV-2 virus have compounded these disparities, likely contributing to increased fatal and nonfatal opioid overdoses specifically and to increased substance abuse behaviors more broadly. Certain racial and socioeconomic demographics have poorer oral health, including non-Hispanic Black individuals and Mexican American adults, who exhibit twice the rates of untreated caries as non-Hispanic White individuals.9 Additionally, low-income or uninsured adults are 3 times more likely to have 4 or more untreated cavities versus adults with higher income levels or dental insurance.9 Similar statistics can be found in the field of pain medicine, with Black patients less likely than White patients to receive analgesic medication for pain, regardless of age or socioeconomic status.9
COVID-19 has not only driven these inequalities but also highlighted the social and economic factors that cause them. Racial and ethnic minorities experienced disproportionately higher rates of COVID-19 infection, hospitalization, and deaths, and the pandemic has also produced disparate effects on socioeconomic conditions in communities of color.9 Take employment as an example. Minority groups have experienced higher rates of job loss. In April 2020, national unemployment rates were 16.7% for Black Americans and 18.9% for Hispanic Americans versus 14.2% for White Americans. Employment status affects a myriad of socioeconomic conditions, such as financial stability, food and housing security, and health insurance coverage—with ensuing impacts on health and dental care.9
Further, pandemic lockdowns also unraveled social safety nets and precipitated a rise in mental health disorders such as anxiety and depression.3 The lockdowns also postponed treatment for substance abuse and similar services while contributing to the death toll—mostly the death of individuals who were already addicted or suffered a relapse that was exacerbated by stress and isolation.3
Opioid Alternatives and Best Practices

 or methadone (T40.3).")
Figure 1. Courtesy of the National Institute on Drug Abuse.10
*Among deaths with drug overdose as the underlying cause, the prescription opioid subcategory was determined by the following ICD-10 multiple cause-of-death codes: natural and semi-synthetic opioids (T40.2) or methadone (T40.3).
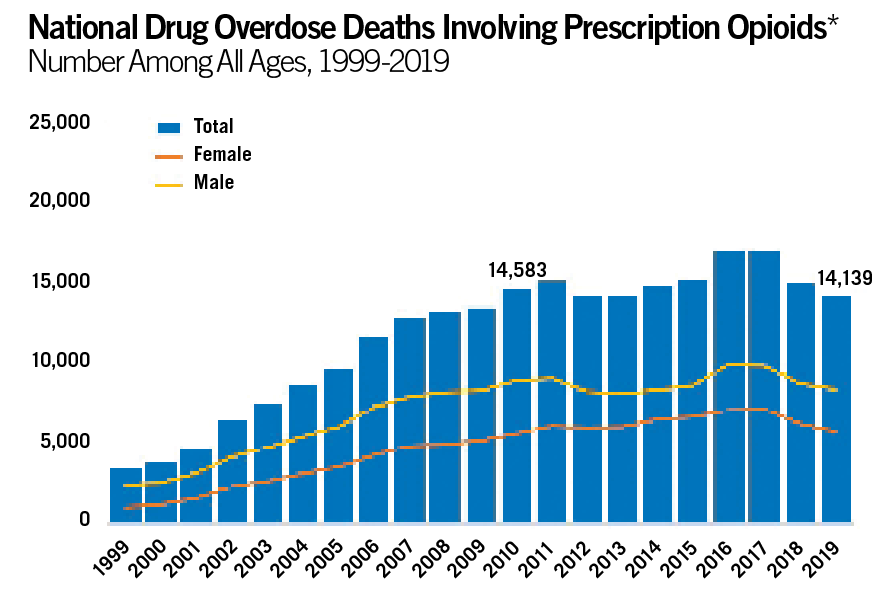
Although the number of deaths due to prescription opioids has been on the decline, deaths due to synthetic opioids have skyrocketed since 2015 (Figure 1).10 Overdose deaths have more than doubled since 2015, with the vast majority caused by synthetic opioids—fueled by rampant use of fentanyl, a fast-acting drug that is 100 times more powerful than morphine.3 The increased use of these synthetic opioids makes it all the more important that dental professionals find alternatives to curb addiction.
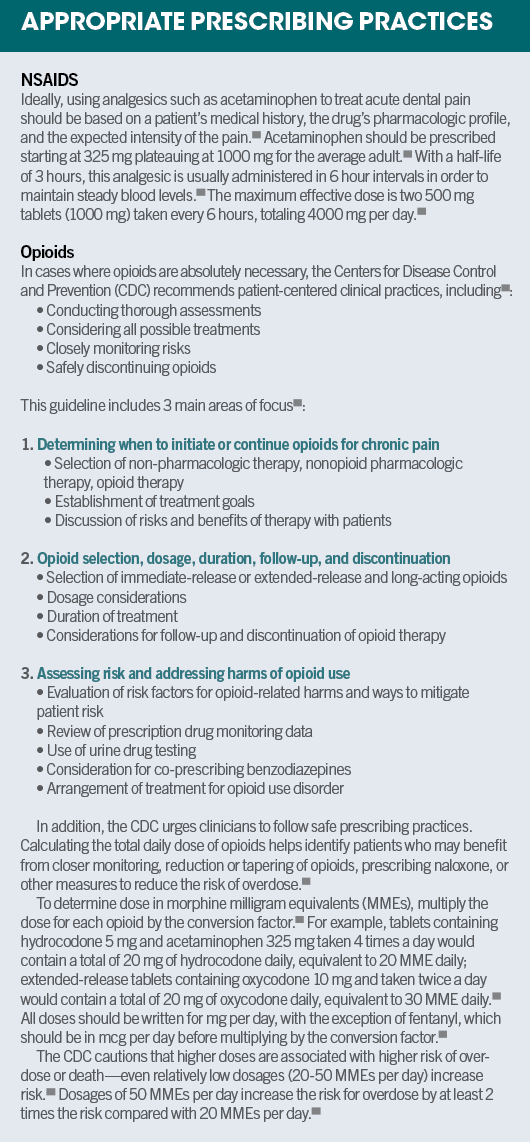
The nonsteroidal anti-inflammatory drugs (NSAIDs) class of analgesic medications is one of the most prescribed, and their effectiveness for treating acute pain has been well proven.11 In addition, nonopioid analgesics such as NSAIDs should be considered the drugs of choice for acute routine pain management, according to the American Dental Association.4
A 2015 systematic review published in the Cochrane Library was a turning point, Dr Jeske says.11
“We became aware of actual quantitative outcomes involving single doses of oral analgesics,” he says. “That was a very important publication because it established the fact that the simple combination of ibuprofen with acetaminophen was actually superior to nearly all opioids and opioid-combination products with acetaminophen. Those findings very much revolutionized our approach to acute postoperative pain control.”
When determining the best pain medication for your patients, it is important to consider the inherent differences in each drug class and to understand dental pain more broadly. NSAIDs reversibly inhibit the enzyme cyclooxygenase (or COX), a precursor to inflammation. NSAIDs also play a role in inflammatory and nociceptive pain processes.11
Opioids, however, bind to specific receptors in the central nervous system, reducing pain perception and pain reaction while increasing pain tolerance.11 They are also associated with a variety of other adverse effects, including drowsiness, respiratory depression, nausea, and vomiting.11
Most dental conditions are inflammatory in nature, so NSAIDs are better suited to treat the specific issue because opioids only mask the pain, Dr Tatch says.
“A lot of times it’s actually counterintuitive to provide opioids because they really do not have a great anti-inflammatory component,” he explains.
Additionally, a combination of acetaminophen and a NSAID has been shown to offer superior analgesic effects to either drug alone with fewer adverse effects or without the possibility for abuse compared with opioids.12


Figure 2. The Vega Recovery kit from StellaLife is formulated as adjunctive therapy for pre- and postsurgical treatment. It includes an antimicrobial rinse, a sublingual spray, and a topical gel.

“I think today, we realize that really very few postoperative dental patients should require narcotics. The appropriate prescribing of analgesics for postoperative dental pain should not include opioids,” Dr Donaldson says.
The use of acetaminophen, with or without the use of a NSAID such as ibuprofen, should be the first line of therapy barring any contraindications, Dr Donaldson adds.
Since 2015, Dr Tatch’s practice has essentially eliminated the use of opioids altogether. “That means that hydrocodone (Vicodin) [and] Percocet [are] not part of our vocabulary when it comes to the postoperative management,” he says. “Occasionally we’ll use a very mild schedule for opioid, like tramadol, just for breakthrough pain.”
In a cohort study of his patients published in the Journal of Oral and Maxillofacial Surgery, Dr Tatch found his practice was able to significantly reduce the percentage of his patients receiving opioids postoperatively. At the start of the study before the restriction on opioids was in place, approximately 2106 patients between the ages of 15 and 85 years underwent surgical procedures, 1184 (59%) of whom required and filled strong opioid prescriptions.13 In 2017, that number was reduced to 19%, even as the number of surgical procedures remained relatively equal.13
“We’ve been able to decrease the number of heavy opioids we prescribe three-fold, which, for a full-scope oral and facial surgery practice, is quite astonishing,” Dr Tatch says. “Our study was published in 2019 and since then, we’ve completely eliminated prescription hydrocodone/oxycontin related medications.
The opioid alternatives Dr Tatch has found success with include NSAIDs, acetaminophen, and the Vega Oral Care Recovery Kit from StellaLife (Figure 2). The kit is a homeopathic medicine that is formulated as adjunctive therapy following surgical treatment. It is said to significantly reduce narcotic pain medications and steroids.
The natural Vega kit includes antimicrobial rinse, sublingual spray, and topical gel. It is indicated for a variety of uses, including all dental surgical procedures such as extractions, bone and tissue grafting, implant placement, and biopsies.
“StellaLife is a wonderful adjunct to postoperative recovery. Not only does it have analgesic properties, but it also accelerates healing,” Dr Tatch says.


Figure 3. First introduced in the US in 2021, Exparel works locally using DepoFoam® delivery technology, which gradually releases bupivacaine over time.

At their endodontics practice in Vermont, Drs Pryles and Blicher also avoid the use of opioids. Instead, they rely on NSAIDs and acetaminophen.
“We know based on the literature that’s available that the single most effective drug for managing postop pain is a combination of ibuprofen and Tylenol,” Dr Pryles says. “That is what I’m recommending, barring any medical history or contraindications, for all of my patients. We know that it works better than anything that’s out there.”
Their office also found that using a local anesthetic as an analgesic can be a good stopgap, especially for patients who are experiencing pain but are not able to be seen immediately, Dr Blicher adds.
“We’ll use a medication called bupivacaine (brand name Marcaine, Septodont), a long-acting anesthetic in the amide family. We administer it the same way,” she explains. “If I have a patient that comes into my office and they’re in tons and tons of pain, and either I can’t see them for a few hours, or they need to get in for an extraction instead—and they can’t be seen for a few hours—we can numb them up.”
If a patient comes in that she feels may have a bit more postoperative discomfort or chronic pain, or even if they cannot take ibuprofen or acetaminophen, Dr Blicher will administer bupivacaine right before treatment to give the patient some relief for a few hours afterward, she says.
Introduced commercially in the United States in 2012, bupivacaine liposome injectable suspension (Exparel) is another alternative that has seen some success, Dr Weinberg says. It is indicated for use at the surgical site to produce a post-surgery analgesia, she explains (Figure 3).


“The research has been done with third-molar models in oral surgery,” Dr Weinberg says. “When they’re doing third-molar extractions with this, it doesn’t diffuse around the inside and the tissues [like] when you’re giving it as a regular local anesthetic in a dental cartridge. So, it’s really a good alternative.”
To ensure you are not writing unnecessary prescriptions, Dr Donaldson suggests that clinicians not practice outside their scope. This includes writing prescriptions for friends and family, he says.
“Just because you have the power of the pen and the authority to write for any prescription doesn’t necessarily mean you should. I sometimes refer to that as the Spider-Man principle: With great power, there must also come great responsibility,” Dr Donaldson says. “You’ve worked too long and too hard for your license. Why would you ever put that at risk?”
In addition, Dr Donaldson recommends that dentists and prescribers follow evidence-based guidelines.
“While you might think, ‘It’s just 1 patient. It’s just 1 prescription. What’s the big deal?’ Eventually, this really does start to add up, and it’s a significant challenge to reverse our course.”
Doctor Education and Patient Expectations
Dental schools and state dental boards have also begun to implement guidelines the past few years around opioid prescribing. Between 2016 and 2020, the University of Colorado School of Dental Medicine took actions to reduce the number of opioids prescribed, and these actions resulted in a 5-step plan14:
- Development of a dental pain management protocol
- Implementation of the protocol with predoctoral students
- Incorporation of the results of a master’s project that determined the actual postoperative pain after periodontal/oral surgical procedures
- Development of a favorite electronic prescription list
- Creation of patient instructions to allow for information on nonopioid analgesic use after dental procedures to be disseminated to the patient
This process resulted in a 68.8% decrease in opioid prescriptions written as well as a 78.6% decrease of opioid pills over this 3-year period.14
“Dental schools have recognized the need for assessing core competencies in pain and anxiety control,” Dr Jeske says. “Certainly, it’s part of our quota accreditation process. And because of that, I believe that most dental schools are now teaching alternatives to opioid analgesics when opioids should not be used or are otherwise contraindicated.”
Things are changing at the state and national levels as well. In 2016, Massachusetts passed a law in an effort to reduce opioid prescription abuse.5 Under this law, students are required to demonstrate how to consider nonopioid treatment options.5
Nationally, the Commission on Dental Accreditation, which sets accreditation standards for all dental schools, required all graduates to be proficient in assessing substance use disorder beginning in 2017.5
Dr Weinberg says she feels that a lack of proper education and awareness on the dangers of opioids may be why some dentists still prescribe opioids when they may not be clinically necessary.
“I think it’s education and not being aware of the other alternatives that are just as good,” Dr Weinberg says. “Hopefully, the younger dentists or dental students are more aware of the risks associated with those drugs and will adapt.”
Continuing education (CE) has a part to play as well. In fact, 24 states mandate CE that is specific to effective pain management, risk assessment for substance use disorder, proper opioid prescribing, naloxone training, regulatory and law enforcement guidelines, and follow-up care, and 7 of those states define course content in specific terms.9
“Just because a medication is over the counter doesn’t mean it’s not as good a pain reliever as the prescribed meds,” Dr Blicher says. “So, we have to have to train our dental workforce to change.”
It is equally important that patients be educated. Many patients are still under the impression that opioids are the best drugs to manage any kind of pain, Dr Pryles explains. Therefore, dentists need to be effective communicators as well.
“Sadly, patients have fallen into some misperceptions as well—that opioids are the best drugs to manage pain,” Dr Pryles says. “My practice counsels patients on the information we have available on these drugs and the fact that they really don’t work to manage acute pain and that we have better alternatives.
“I think a lot of what we need to do now is manage patients’ expectations,” she continues. “Sometimes postop soreness is normal, and we can minimize it with drugs. Sometimes being pain-free is not a realistic expectation. But we can certainly keep people comfortable and do so reasonably well with these over-the-counter meds.”
Many patients believe the misconception that they will get better pain relief from a controlled substance, Dr Jeske says. In fact, “controlled substance” simply refers to a drug’s tolerance and potential for addiction, he explains.
“That creates in the mind of the patient a perception that they will get better pain relief because it is, in fact, a controlled substance,” Dr Jeske says. “Whereas the actual classification as a controlled substance simply refers to the ability of the drug to produce tolerance and dependence leading to addiction. So just because a drug is classified as a controlled substance does not imply, should not imply, that it is pharmacologically superior to a noncontrolled substance.”
With high patient expectations comes the likelihood that patients will request something stronger than Tylenol, Dr Donaldson adds.
“Sometimes, the dentist will fall into that trap of prescribing what the patient tells [them] to prescribe—which I always warn against,” Dr Donaldson says. “[You’ve] got a waiting room full of other patients, and do you want to spend a lot of time counseling this individual as to why you’re not going to prescribe an opioid? Or is it easier just to write that Vicodin prescription and get them out of your office and get on to the next case? So, they have a lot of pressures from many areas to succeed in this field.”
Patient feedback can be valuable information. Dentists should ask what their patients usually take for pain before writing a prescription, Dr Weinberg says. This can help clinicians narrow down medications to find something that will be effective, and it can give clinicians confidence that the prescriptions they write will help alleviate their patient’s pain.
Antibiotic Prescriptions on the Rise
It isn’t just opioids being overprescribed in dentistry. An increase in antibiotics prescribed has been tracked over the past several years, according to a study published in the American Journal of Preventive Medicine.7
This study found that while opioid prescription rates have declined by 20%, antibiotic prescriptions have increased by 5%.7 Both Drs Pryles and Blicher have seen this play out in their practice. Although antibiotics are an incredibly powerful tool for dental professionals, they are still drugs that clinicians must use responsibly and only when appropriate, Dr Pryles says.
“Anecdotally, from my own practice and also chatting with endodontic colleagues, the number of patients I see every day that come in having been prescribed an antibiotic inappropriately to treat inflammation, the numbers are staggering,” Dr Pryles says. “And what we’re seeing as a result of that...is a significant increase in the numbers of resistant infections—infections that are getting harder to treat or sometimes nearly impossible to treat with the oral antibiotics that we have at our disposal.”
If this trend is not countered, dental and medical professionals alike could see these medications become less and less effective against infections as resistance to these drugs builds, she notes.
Additionally, antibiotics come with their own adverse effects, Dr Jeske says. “Unfortunately, some of the antibiotics that we prescribe in dentistry—which are very effective—are also associated with a higher incidence of adverse gastrointestinal effects,” he explains.
One of the more common adverse effects of antibiotics is Clostridioides difficile, an infection of the large intestine. A severe C difficile infection can lead to hospitalization. Common symptoms include dehydration, abdominal cramping, and kidney failure.15
Amoxicillin is one of the most frequently prescribed antibiotics, Dr Weinberg says. Because amoxicillin is a broad-spectrum antibiotic, it has unintended consequences, she explains.
“The extra bacteria that it gets has nothing to do with dental infections,” Dr Weinberg says. “The broader you go, the more [adverse] effects you have. You lose your good bacteria.”
Instead, she recommends dentists use penicillin V potassium (Penicillin VK), which is a more narrow-spectrum drug.
Moving Forward
To help curb the heavy reliance on opioids, it’s key for the dental industry to recognize the role that it has played and make significant changes to its prescribing habits.
It is also critical that dental prescribers follow evidence-based best practices and regulations and recommendations set by their state dental boards and the Centers for Disease Control and Prevention, Dr Donaldson says.
“If we continue to consider high-level scientific evidence for acute postoperative pain control, then we will begin to curtail the total amounts of analgesics that we’re prescribing,” Dr Jeske says. “And in many cases, we are able to do that without having to prescribe opioids.”
References
- Baker DW. The Joint Commission’s pain standards: origins and evolution. May 5, 2017. Accessed Nov. 9, 2021. https://www.jointcommission.org/-/media/tjc/documents/resources/pain-management/pain_std_history_web_version_05122017pdf.pdf?db=web&hash=E7D12A5C3BE9DF031F3D8FE0D8509580&hash=E7D12A5C3BE9DF031F3D8FE0D8509580
- Drug overdose deaths. The Centers for Disease Control and Prevention. Last reviewed March 3, 2021. Accessed November 8, 2021. https://www.cdc.gov/drugoverdose/deaths/index.html
- Rabin RC. Overdose deaths reached record high as pandemic spread. New York Times. November 17, 2021. Accessed November 18, 2021. https://www.nytimes.com/2021/11/17/health/drug-overdoses-fentanyl-deaths.html
- Suda KJ , Zhou J, Rowan SA, McGregor JC, et al. Overprescribing of opioids to adults by dentists in the U.S., 2011–2015. American Journal of Preventive Medicine. 58(4) 473-486. 2020. doi.org/10.1016/j.amepre.2019.11.006. Accessed October 28, 2021. https://www.sciencedirect.com/science/article/pii/S0749379719305276
- R Siegel, J Cheung. Dental schools add an urgent lesson: Think twice about prescribing opioids. NPR. September 8, 2017. Accessed October 28, 2021. https://www.npr.org/sections/health-shots/2017/09/08/549218604/dental-schools-add-an-urgent-lesson-think-twice-about-prescribing-opioids
- Okunev I, Frantsve-Hawley J, Tranby E. Trends in national opioid prescribing for dental procedures among patients enrolled in Medicaid. Journal of the American Dental Association.152(8) 622-630. August 1, 2021. Accessed October 27, 2021. https://jada.ada.org/article/S0002-8177(21)00244-0/fulltext
- Hubbard CC, Evans CT, Calip GS, et al. Characteristics associated with opioid and antibiotic prescribing by dentists. American Journal of Preventive Medicine. 60(5) 648-657. May 2021. Accessed October 27, 2021. doi.org/10.1016/j.amepre.2020.11.017
- Schroeder AR, Dehghan M, Newman TB, Bentley JP, Park KT. Association of opioid prescriptions from dental clinicians for US adolescents and young adults with subsequent opioid use and abuse. JAMA Intern Med. 2019;179(2):145–152. doi:10.1001/jamainternmed.2018.5419 Accessed November 19, 2021. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2717503
- Scrivani SJ, Keith DA, Kulich RJ, et al. Pain management for dental medicine in 2021: Opioids, coronavirus and beyond. J Pain Res. 2021;14:1371-1387. Accessed November 1, 2021. https://doi.org/10.2147/JPR.S319373
- Overdose death rates. National Institute on Drug Abuse. Updated January 29, 2021. Accessed October 28, 2021. https://www.drugabuse.gov/drug-topics/trends-statistics/overdose-death-rates
- Moore RA, Derry S, Aldington D, Wiffen PJ. Single dose oral analgesics for acute postoperative pain in adults - an overview of Cochrane reviews. Cochrane Database Syst Rev. 2015;2015(9):CD008659. Published 2015 Sep 28. doi:10.1002/14651858.CD008659.pub3
- Donaldson M, Dickinson S, Goodchild J. Inside Dentistry. Jan 2017. 13(1) 1-2. Accessed November 1, 2021. https://www.aegisdentalnetwork.com/id/2017/01/prescribing-opioids-after-dental-treatment
- Tatch W. Opioid prescribing can be reduced in oral and maxillofacial surgery practice. Journal of Oral and Maxillofacial Surgery. 77(9):1771-1795. September 1, 2019. Accessed November 9, 2021. doi.org/10.1016/j.joms.2019.03.009
- Font K, Johnson L, Powell C. Five different solutions to mitigate overprescribing opioid medications. J Dent Ed. August 2020. 85:31-36. Accessed November 3, 2021. https://onlinelibrary.wiley.com/doi/epdf/10.1002/jdd.12393
- C. difficile infection. Mayo Clinic. Updated August 27, 2021. Accessed November 4, 2021. https://www.mayoclinic.org/diseases-conditions/c-difficile/symptoms-causes/syc-20351691
















