REVIEW: Premier Dental's T-LOC™ dual-arch impression trays rank high for patient comfort, ease of use
The Catapult Group reviews the T-LOC Triple Tray adhesive-free, dual-arch impression tray
The Catapult Group reviews the T-LOC Triple Tray adhesive-free, dual-arch impression tray



The excellence and marginal fit of the definitive laboratory restorations can only be as good as the master dies from which they are created. The precision of the master impression is something that cannot be compromised.
Marginal detail and tooth structure apical to the restorative margin are both necessary elements of an acceptable final impression. Without precision, the definitive restoration is doomed to clinical failure. Remember in dental school hearing, “Let’s pour it up and see what we’ve got.” If you can’t see the margins in the impression, they won’t “magically” appear when the impression is poured. It is important for the dentist to have a critical eye and reject all but the “perfect” master impression.
Preparation of the gingival tissues: The Two-Cord Technique

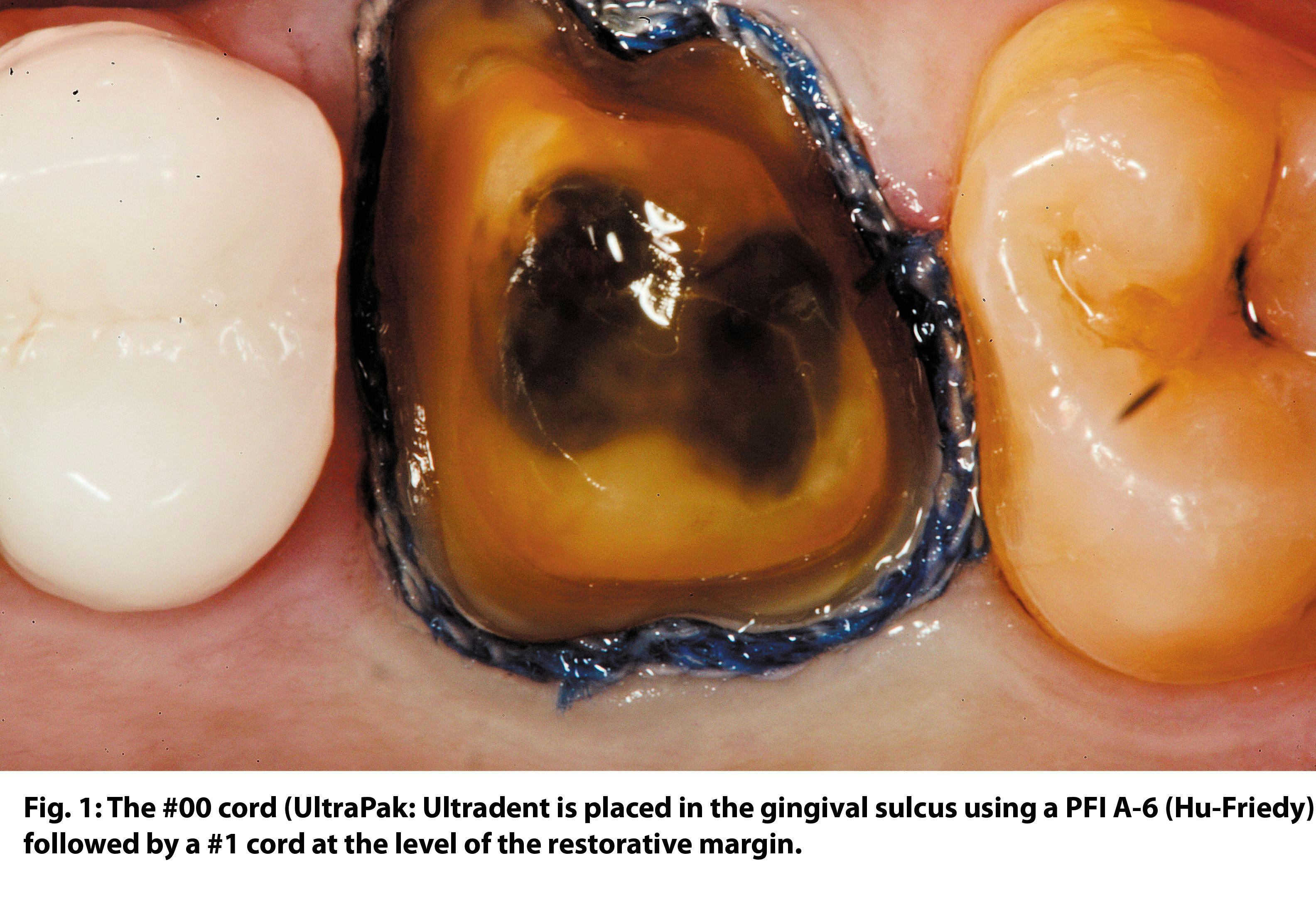
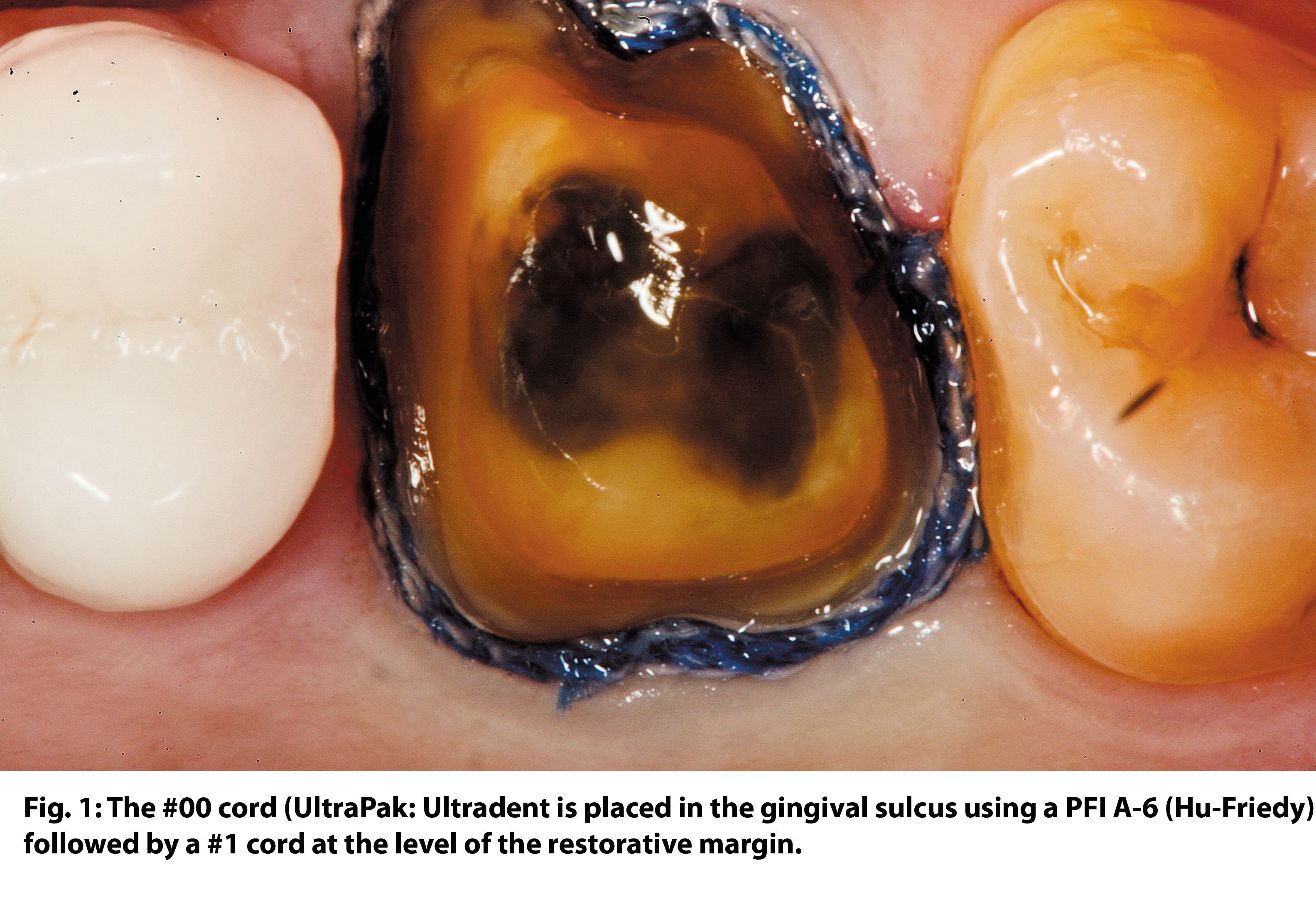
A two-cord impression technique is used to capture most master impressions for full coverage (circumcoronal) and facial veneer restorations with both intracrevicular and equicrevicular margins (at the free gingival margin). First, a #00 cord soaked in Hemodent (Premier USA) is packed around each preparation margin starting from the lingual proximal to the facial aspect, then back through the remaining proximal area to the lingual aspect. The excess at both lingual ends is trimmed, and the ends of the cord are tucked into the lingual gingival sulcus so the ends butt against one another. Next, a #1 cord is placed on top of the #00 in the same fashion as previously described (Fig. 1 - click to enlarge).
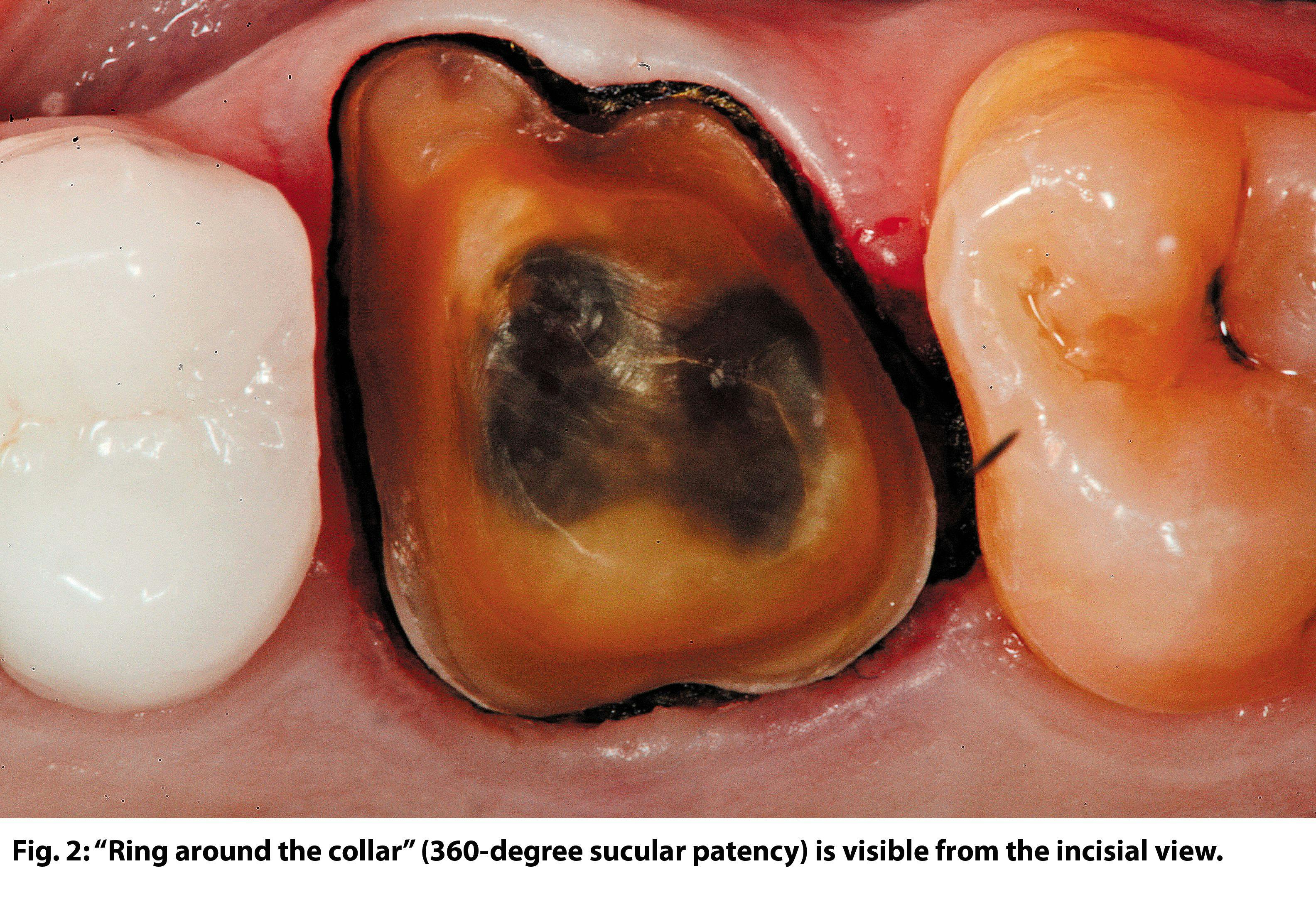
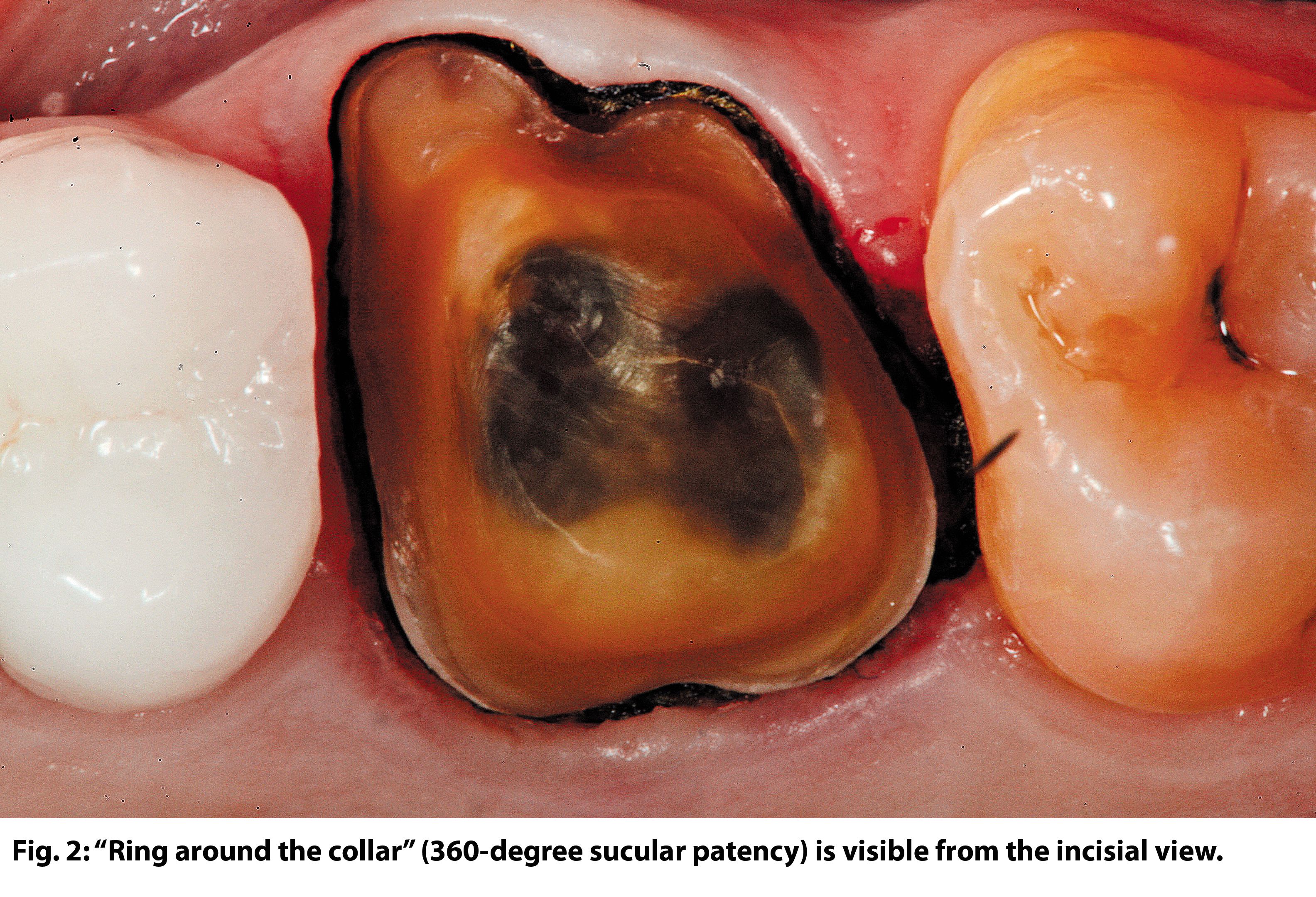
The preparation is cleansed with AcQuaSeal Dentin Desensitizer (AcQuaMed Technologies) on a cotton pledget. When ready, the #1 cord is teased out of the sulcus using an explorer, from the facial aspect of each preparation and the amount of retraction is evaluated. The impression should capture not only the entire restorative margin, but also about 0.5 millimeters of the tooth/root surface apical to the margin (Fig. 2 - click to enlarge).
If the marginal gingiva adjacent to any restorative margin rebounds to contact the tooth/margin, a small piece of a larger diameter cord (#2) is placed into the affected area for an additional minute, and then removed. This should be sufficient to create a space between the tooth surface and the inner lining of the gingival sulcus.
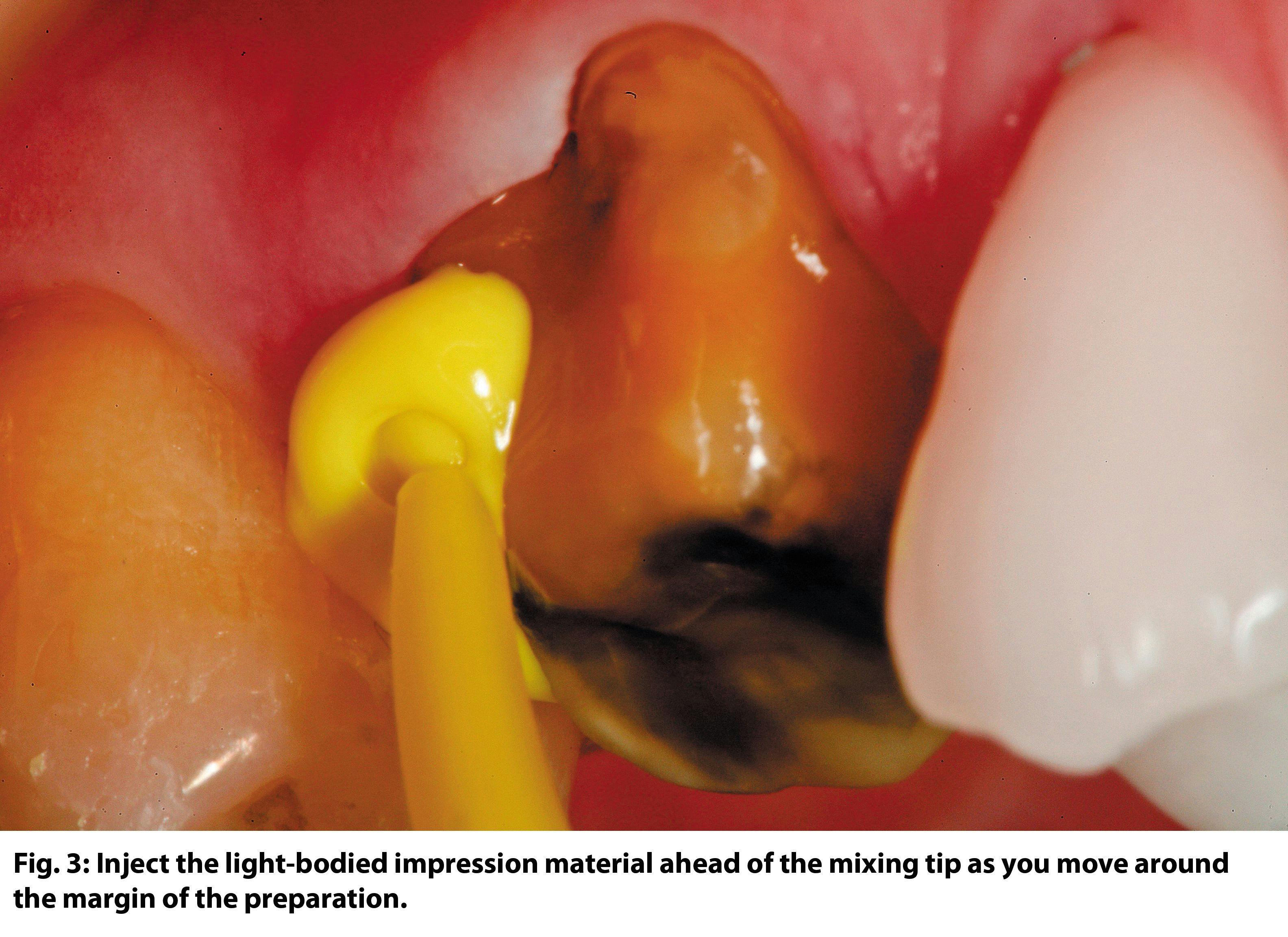
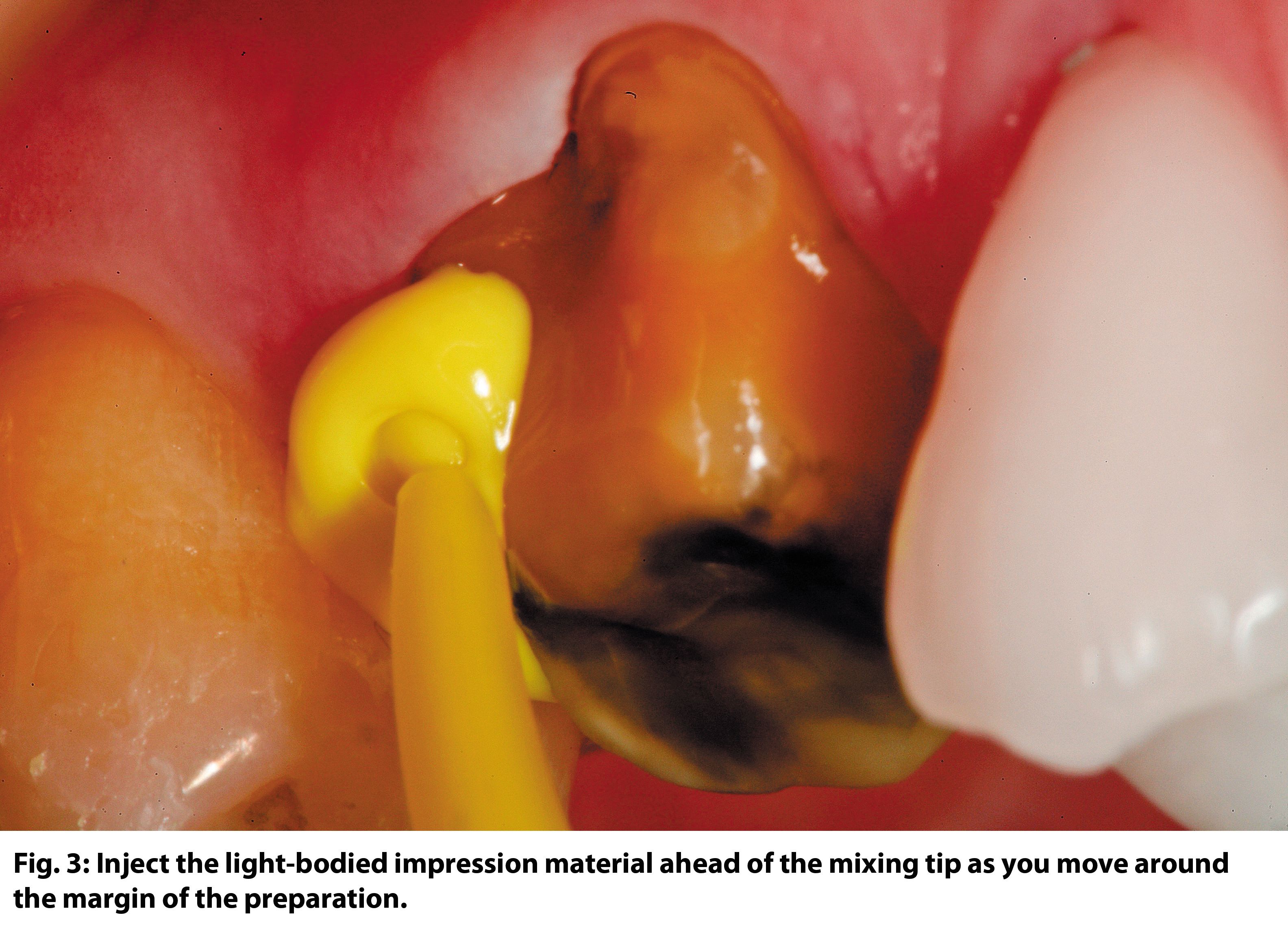
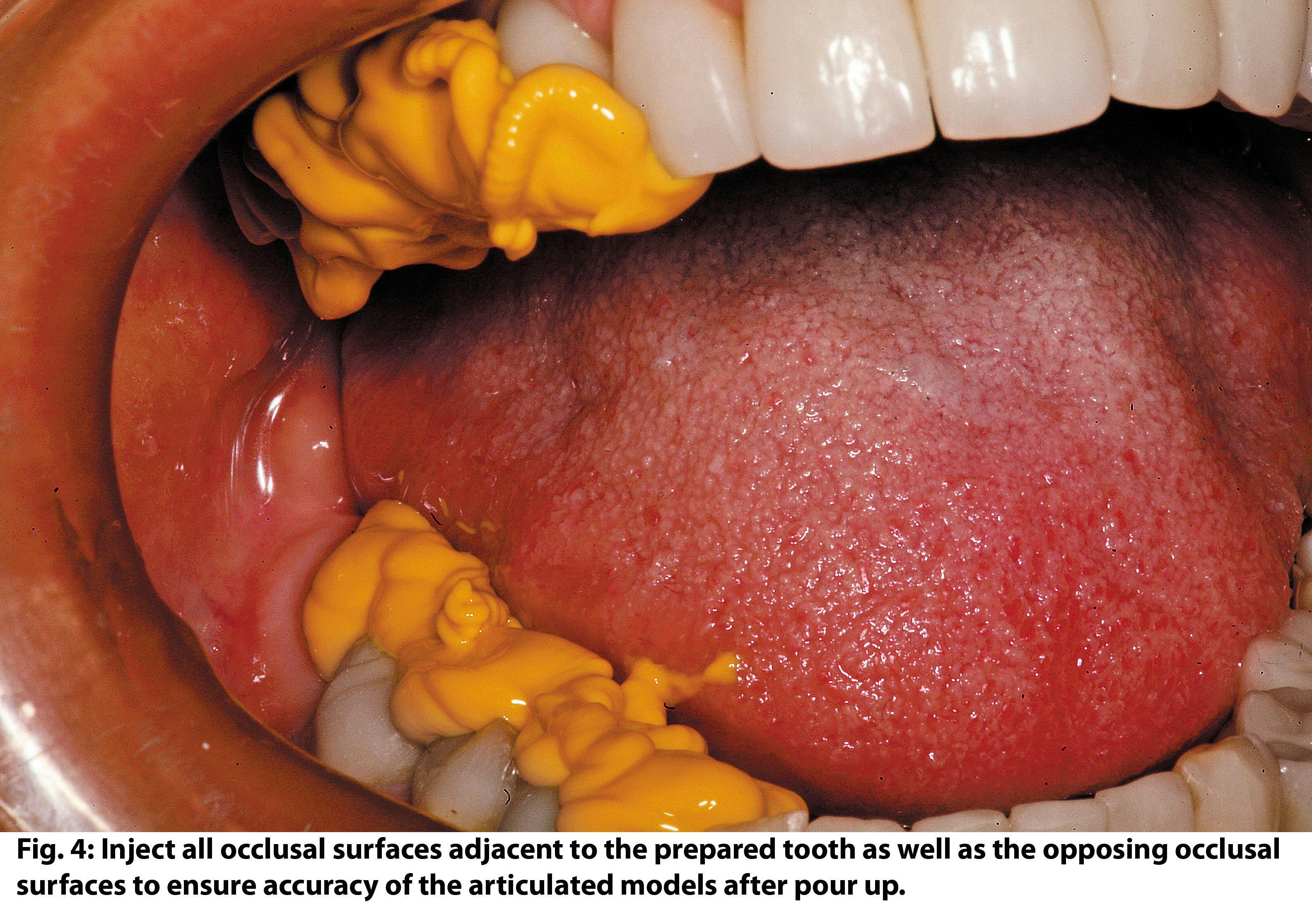
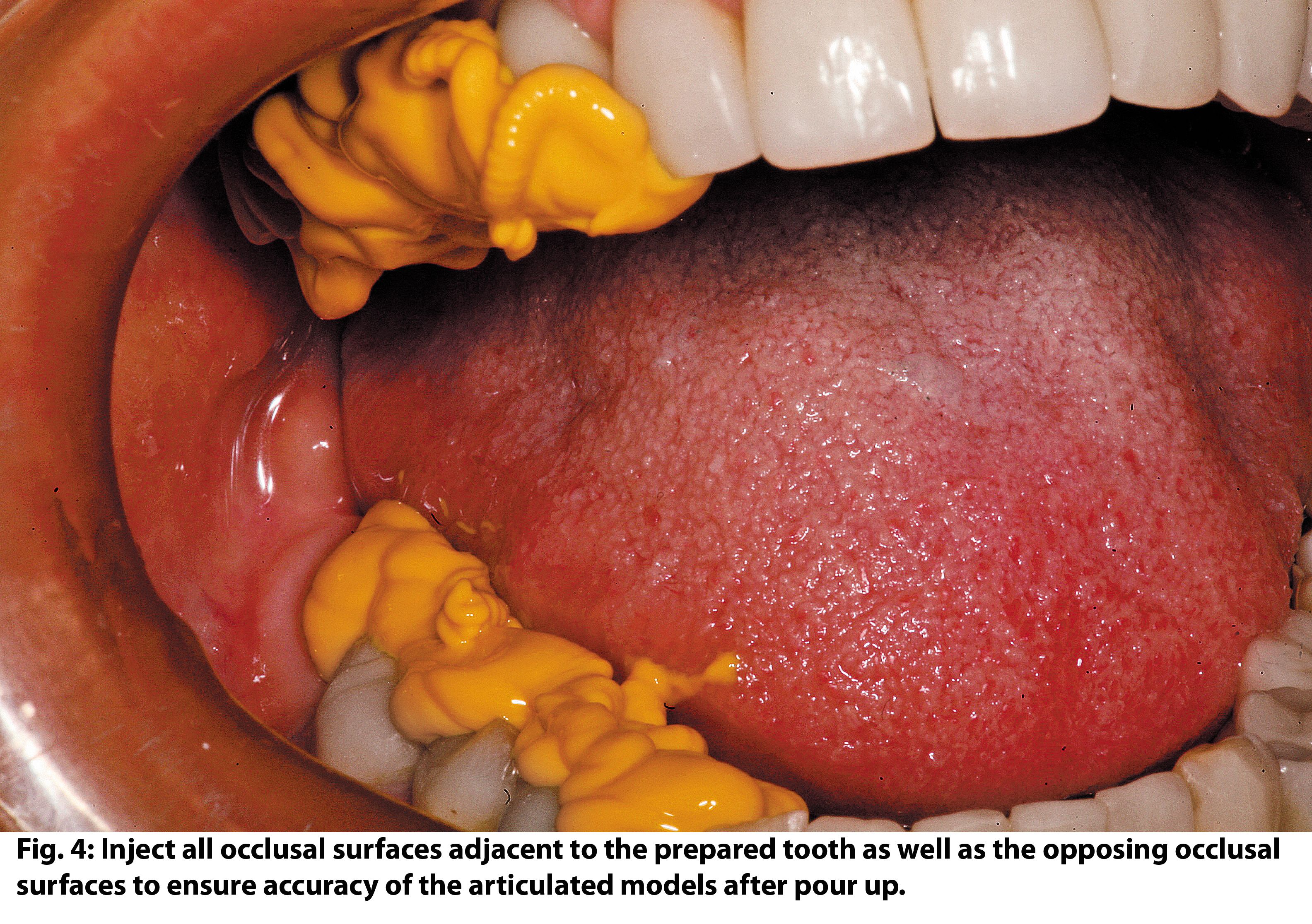
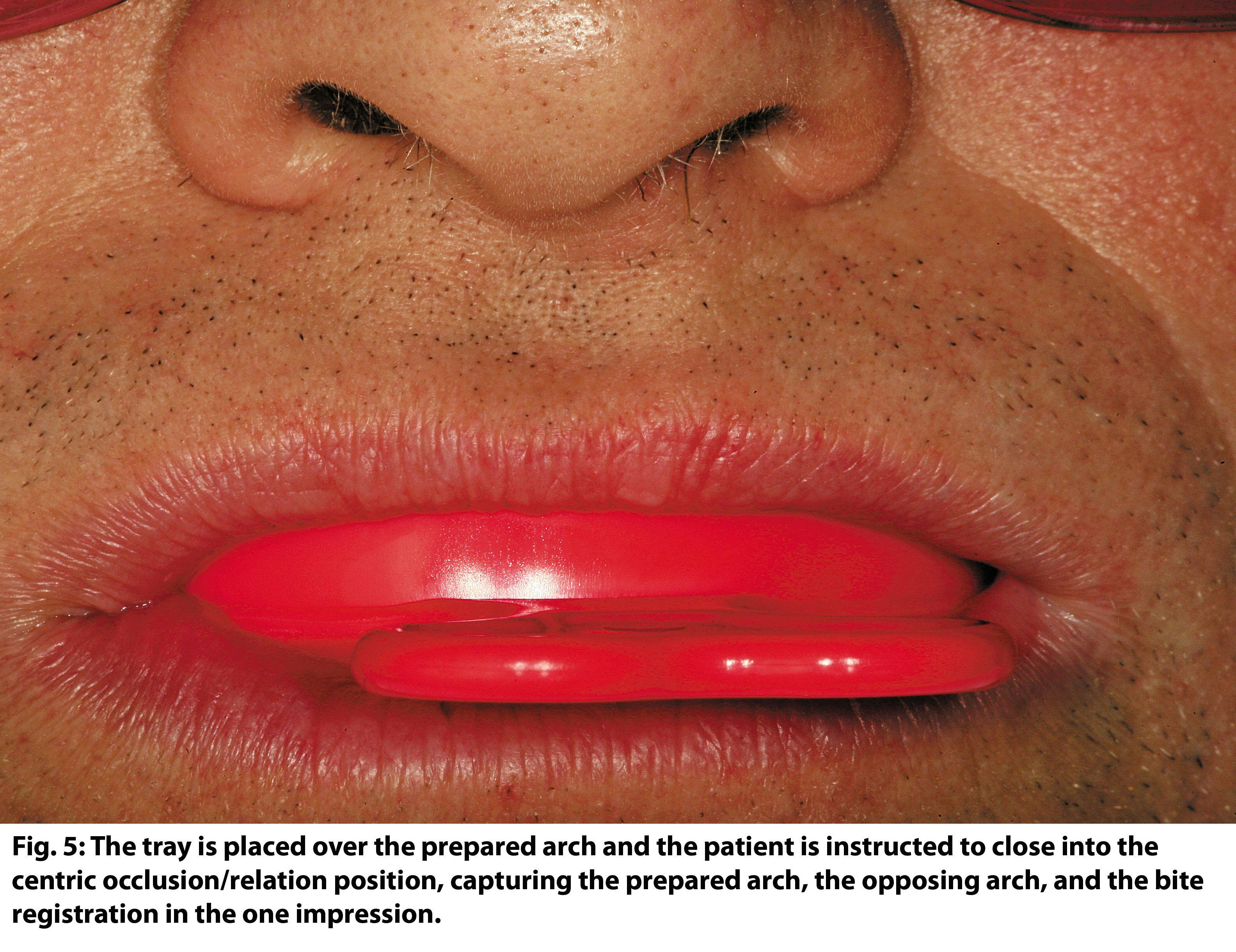
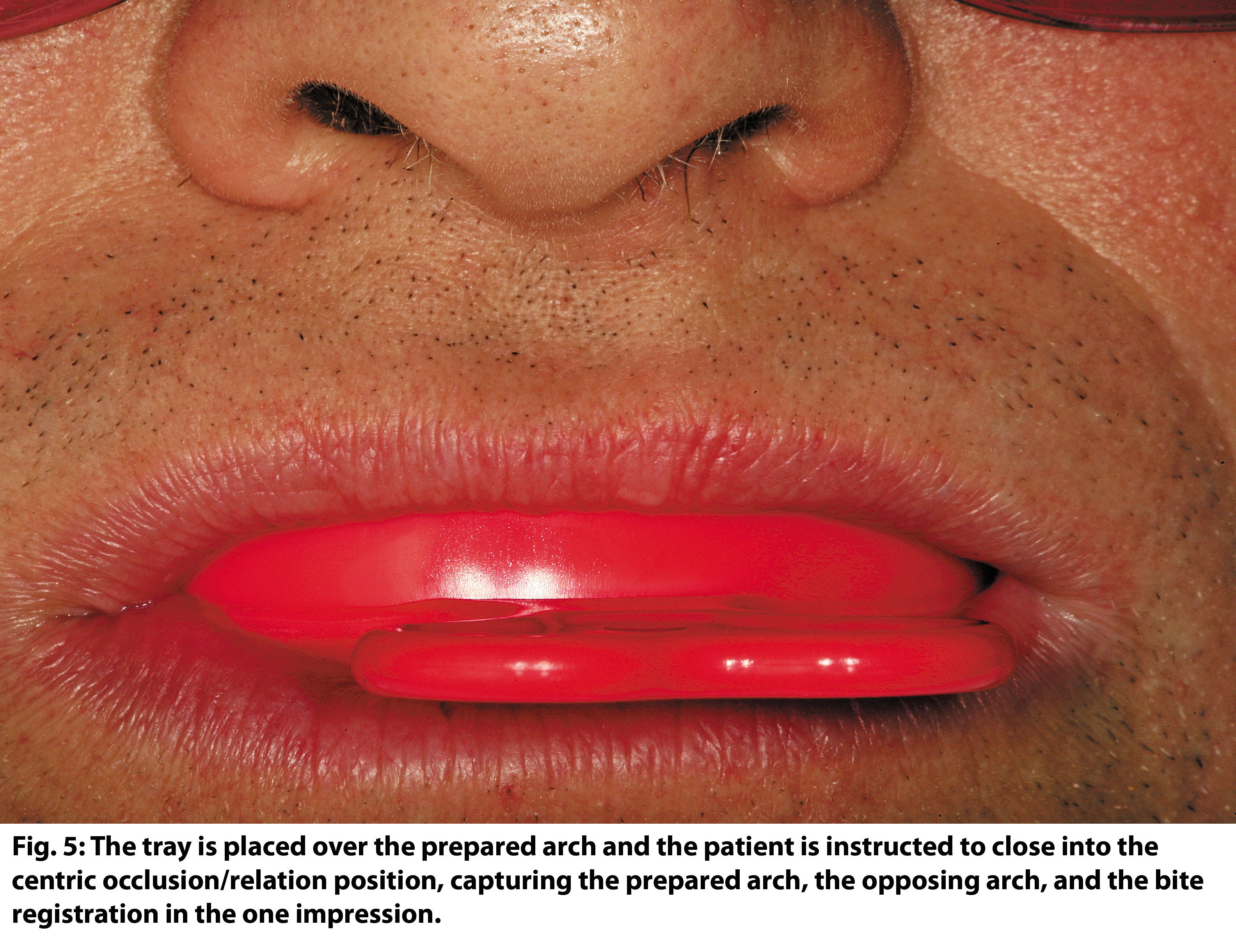
The goal of retraction is to “create a moat (space in which to inject light bodied impression material) around the castle (tooth preparation).” To capture a precision impression, light bodied impression material should be injected not only around the prepared teeth (Fig. 3 - click to enlarge), but also over all occlusal and incisal surfaces so the stone models can be accurately articulated (Fig. 4 - click to enlarge). The impression tray with the heavy bodied impression material is then placed in the mouth (Fig. 5 - click to enlarge) for the appropriate time based on manufacturers’ recommendations.




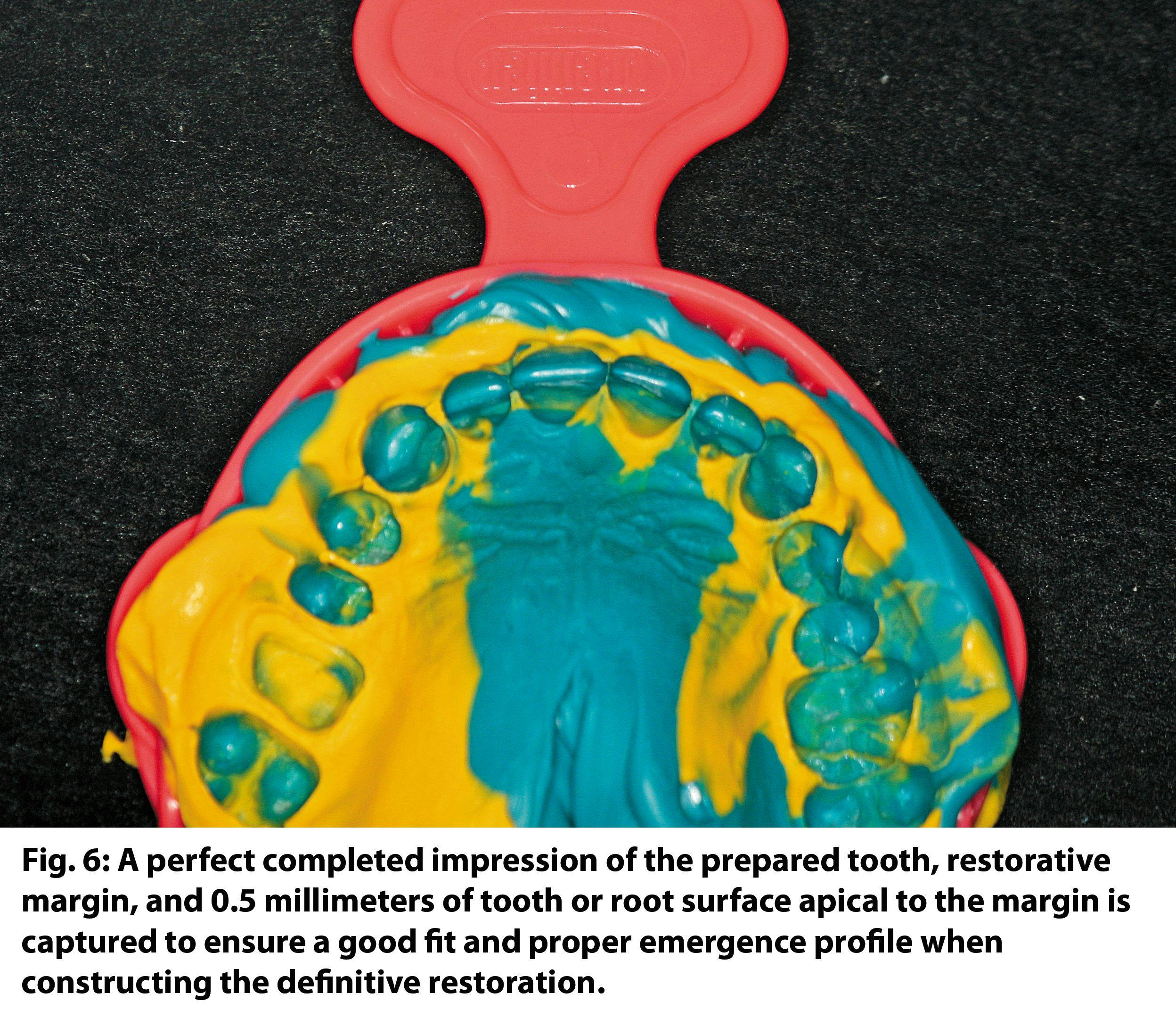
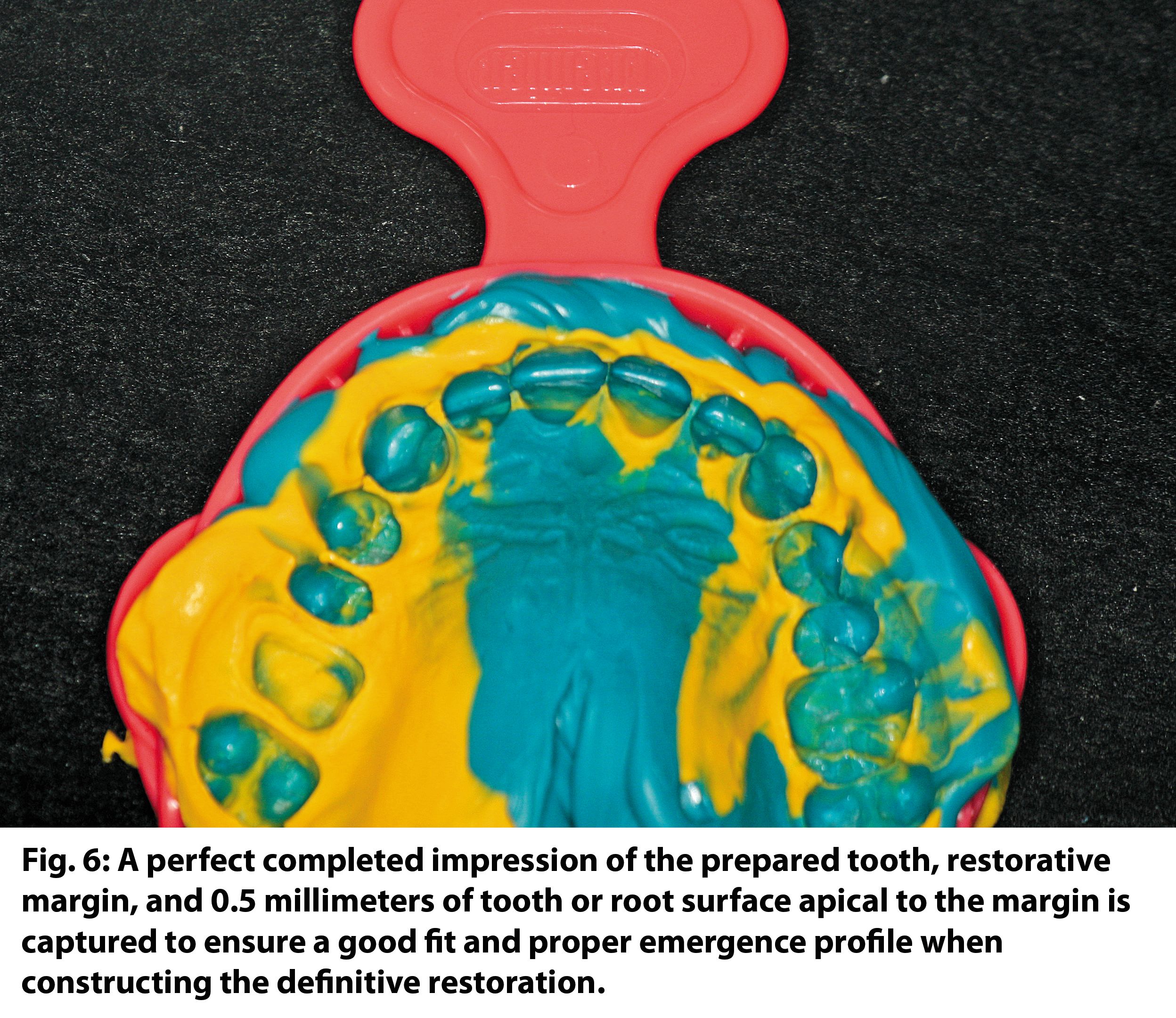
When inspecting the master impression, all preparation margins should be readily visible and a cuff of impression material must appear around all marginal areas (Fig. 6 - click to enlarge). This will help to ensure proper marginal trimming of dies by the laboratory and correct restorative emergence profiles.
The role of the impression tray
The role of the impression tray is to deliver the impression material to the oral cavity and support it while it sets around the teeth. “Triple Tray,” “Double Bite,” or “Quad Bite” types of trays are designed to capture the prepared arch, the opposing arch, and the bite registration in one impression and can be used for one or two unit cases when there is a centric holding stop both mesial and distal to the prepared area. An example of this type of tray is T-LOCTM Triple Tray® from Premier Dental Products. According to the manufacturer, some of the features of this tray include:
- Ultra thin webbing ensures accurate bite registration by allowing precise interdigitation of the opposing teeth.
- Patented retention tracks lock in the impression material for accuracy without the use of adhesives.
- Large, ergonomic handles allow for easy transfer between the assistant and dentist.
- Being disposable, T-LOC trays are aseptic. There is no cleaning or sterilizing involved in use.
Catapult Group evaluation
Premier’s new 3/4 Arch T-LOC tray received a very good evaluation and is a nice addition to the anterior and posterior T-LOC tray family. The group uses a very wide variety of impression material systems but had good results across those systems. More than 70% of the group would recommend this tray in their lectures for at least some impression procedures.
The tray received very high marks for its ease of use, speed of use and relative rigidity. Having said that the only caveats to full recommendation were some reservations that were expressed about the consistent accuracy of the tray and how “spring back” might lead to less than optimal results. Of course this concern would be inherent in almost any double arch tray system and likely could only be addressed with a custom or metal single arch tray technique.
Some of the evaluator comments included:
- “Comfortable for the patient”
- “Very simple to use, quite stable”
- “The plastic of the trays was sturdy enough to yield accurate impressions and easy to use.”
- “Better occlusion”
- “Good rigidity and higher sides for more depth of material”
Clinical situations in which to use T-LOC 3⁄4 Arch Anterior Trays
- Single unit posterior crowns
- Smaller anterior cases where you need more posterior occlusion but full arch not required
- Adjacent single units
- C&B & implant impressions
Conclusion: 100% or 0%
There is no “almost” in taking the perfect master impression. Control of the gingival tissues through precise provisionalization, proper tissue retraction, and use of a quality impression tray will ensure repeatable excellence in this most critical step of dental reconstruction.
ABOUT CATAPULT



Catapult is an organization that consists of more than 50 clinicians spread throughout Canada and the United States. As a company, manufacturers pay a fee for their product to be evaluated and what we deliver are truthful, independent answers from surveys that we develop with them. We have had many products that have either had to be altered before hitting the market or simply never arrived because of our openly honest evaluations. In this way, Catapult assists the manufacturer to avoid potentially releasing a faulty product, or simply a product that needs refinement. Lastly our clients are omnipresent in the industry, small to large, no favoritism, simply reviewing the latest products in our practices.










