How to use Magnetic Max in conservative implant surgery
How the Magnetic Max provides essential surgical advantages as well as greater patient satisfaction.



The Magnetic Max is a magneto-dynamical instrument assembled into a handpiece energized by a power control device, delivering forces by timing of application. The osteotomes are attached to the handpiece that push a shock wave on their tip. This gear is useful for root extraction and bone volume expansion to avoid distress symptoms claimed by patients when a hand mallet is used.
Magnetic Max exploits an electro-magnetic, electronically-operated collision between two masses, allowing a high-intensity impact to be applied in a very short timing; all that permits you to get an elastic wave, followed by a quantity of motion, which expresses itself in an inelastic shock wave on the bone. This lets you obtain the plastic deformation of the bone.
The Magnetic Max imparts to osteotomes a longitudinal movement along the central axis, moving up and down toward the pilot bone hole, providing a driving mechanism of longitudinal movements.
Trending : How to match any composite restoration shade
Such mechanical sequence of osteotomes progressively condensed internal bone wall of initial hole radially outward with respect to central axis to create high-density bone tissue along a substantial portion of the length of the implant site preparation.
The Magnetic Max (Figs. 1-2) is useful for conservative root extraction.

Fig. 1



Fig. 2

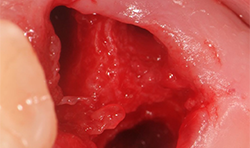
Fig. 3
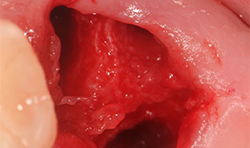
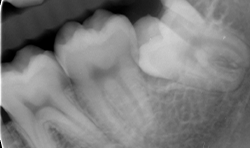
Fig. 4a
Maximum preservation of the alveolar housing and related gingival structures may be achieved following assisted atraumatic tooth extraction by an electrical mallet (Fig. 3).
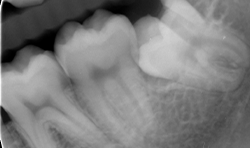
Different thin metallic blades may be connected to the Magnetic Max handpiece, sending a magnetic wave on the tip. The Magnetic Max imparted to blade a longitudinal movement along the central axis, moving up and down between root surface and lamina dura of the alveolus in a repetitive circumferential fashion, providing a driving mechanism of longitudinal movements. This movement also allows the maintenance of lamina dura for wisdom teeth (Figs. 4a-4c).
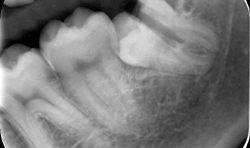
Fig. 4b
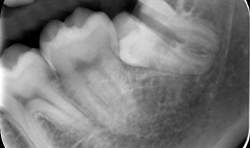
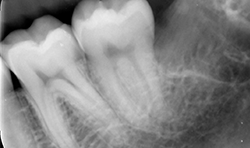
Fig. 4c
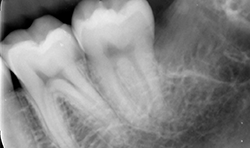
Fig. 4b Fig. 4c
The aim of conservative implant surgery is to create a surgical site for implants by displacing a portion of native residual bone using blades and osteotomes pushed by Magnetic Max (Figs. 5a-5e).


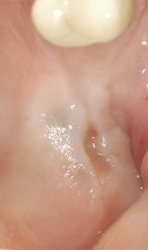

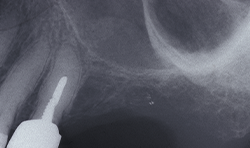
Fig. 5a Fig. 5b
In osteotome-assisted surgery for a sinus lift procedure, the use of Magnetic Max provides some essential advantages during the surgical procedure in comparison with a hand mallet. Magnetic Max supplies a more precise control of osteotome of the entry direction (or directionality) of the tip into the bone. This is an important concept because bone is generally formed of parts with different density, and the expander tends to be deflected when it moves from a bone part with a specific density to another bone part with a different density.

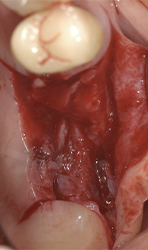

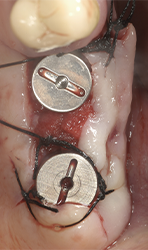
Fig. 5c Fig. 5d
Furthermore, the handling of the magnetic device is very simple because the mechanical oscillations generated by the actuator, which are transmitted via the hydraulic linkage to the osteotome, are transmitted without difficulties to the workpiece.

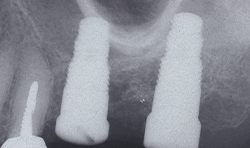
Fig. 5e
In cases with few residual bones in the posterior maxilla, osteotome with Magnetic Max are useful for transcrestal maxillary sinus floor elevation. Its aim is to create a surgical site for implants by displacing a portion of native residual below bone within the cavity of the maxillary sinus. This particular type of bone is usually found below the sinus floor and, through this technique, is displaced vertically in order to create a new implant alveolar portion.
In the final configuration of the surgically created alveolus, the coronal portion of the crest must give primary implant stability. This will be completed by the coronal bone portion pushed laterally and internally of the sinus cavity, from which a sort of closed “tent” formed by the sinus membrane will keep the cavity closed.
Continue reading on page two...
The osteotomy is gradually expanded in 0.5 mm increments using osteotomes inserted to the working depth. The final diameter of the osteotomy is 1.2 mm less than the anticipated implant diameter, depending on local bone density.




Fig. 6a Fig. 6b
Such mechanical sequence of osteotomes progressively condensed internal bone wall of initial hole radially outward with respect to central axis to create high-density bone tissue along a substantial portion of the length of the implant site preparation. The platform of the implants is inserted at the level of the alveolar crest. A minimum insertion torque of 30 Ncm is considered.



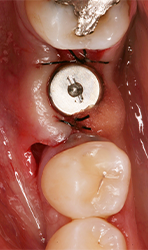
Fig. 6c Fig. 6d
Subsequently, the soft tissues are sutured. The buccal flap is apically repositioned and stabilized with sutures tied to the margin of the palatal flap and anchored buccally with a loose loop to the periosteum at the level of the alveolar mucosa. This suture design avoids tissue traction in the repositioned buccal flap. The gap between the superficial margin of the buccally repositioned tissue and lower part of the palatal tissue, healed by secondary intention in order to increase the size of keratinized mucosa.
Related reading: How to perform a void-free restoration
The goal is to change the height of available bone by creating an osteotomy tunnel starting from the crestal position and extending, initially transversally and medially, in a direction parallel to the palatine vault.


Fig. 6e
Ridge split with Magnetic Max represents a predictable surgical procedure, doesn’t lead to bone injury and doesn’t lead to bone overheating. This surgical technique is rendered safe, less technique sensitive, comfortable and without risk of any form of vertigo (Figs 6a-6e).
The Magnetic Max device had a better bone condensing efficiency, especially in softer bone, because of the magnetic wave and the subsequent shock wave; induced axial and radial movements applied on the tip of the osteotome with a fast energy prevents patient distress. However, further clinical trials are mandatory to evaluate the efficiency of this new device for osteotome procedure, but these results encourage the development and continuation of this technique.
"It is a rare thing in dentisty where a technology comes along that so revolutionizes the way we practice. The Magnetic Max has done just this. The comfort level for my patients is unparalleled compared to other procedures!" says Dr. Joseph Maniscalco, prosthodontist Brooklyn, New York.
References
1. Roberto Crespi, Giovanni B. Bruschi, Paolo Capparè, Enrico Gherlone. The Utility of the Electric Mallet. The Journal of Craniofacial Surgery. 2013.
2. Roberto Crespi. Magnetic Max in bone remodeling. Quintessence ed. 2016.
3. Roberto Crespi, Paolo Capparè, Enrico Gherlone. Electrical Mallet Provides EssentialAdvantages in Maxillary Bone Condensing. A Prospective Clinical Study. Clin ImplantDent Relat Res. 2013; 15(6): 874-82. doi: 10.1111/j.1708-8208.2011.00432.x.
4. Roberto Crespi, Paolo Capparè, Enrico Gherlone. Sinus Floor Elevation By Osteotome. Hand Mallet Versus Electrical Mallet. A Prospective Clinical Study. Int J Oral Maxillofac Implants 2012 Sep-Oct;27(5):1144-50.
5. Roberto Crespi, Paolo Capparè, Enrico Gherlone. A Comparison Of Manual And Electrical Mallet In Maxillary Bone Condensing For Immediately Loaded Implants: A Randomized Study. Clin Implant Dent Relat Res. 2014; 16(3): 374-82. doi: 10.1111/j.1708-8208.2012.00485.
6. Crespi R, Capparè P, Gherlone E. Electric Mallet In Implants Placed In Fresh Extraction Sockets With Simultaneous Osteotome Sinus Floor Elevation. Int J Oral Maxillofac Implants. 2013 May-Jun;28(3):869-74.
7. Crespi R, Capparè P, Gherlone E. Ewlectrical Mallet Provides Essential Advantages In Split-Crest And Immediate Implant Placement. Oral Maxillofac Surg. 2014 Mar;18(1):59-64.
















