Successful Endo With Outcomes-Based Treatment Planning
Prognostic data are fundamental to case selection and can help both clinicians and patients make educated choices regarding the optimal strategies for individualized endodontic care.


ALEXANDR MITIUC / STOCK.ADOBE.COM
This article focuses on outcomes as a means to aid practitioners in treatment planning for endodontics procedures; specifically, the ways in which clinical prognostic factors can affect outcomes for our “big 3”—nonsurgical root canal therapy, nonsurgical retreatment, and apical microsurgery endodontic procedures.
An understanding of outcomes is fundamental to diagnosis and treatment planning in endodontics. Although some patients are often initially concerned about whether proposed treatment options are going to hurt, many are far more focused on the predictability and reliability of endodontic treatment. Treating clinicians must not only evaluate risk based on clinical and radiographic findings but also communicate both the risks and benefits of all treatment options as part of informed consent. Much of the conversation about risk centers around outcomes data and the factors that affect those outcomes.
Though extraction, informed refusal, and vital pulp therapy may be alternative options, treatment plans for endodontic pathology frequently include the “big 3” procedures within the specialty’s scope: nonsurgical root canal therapy, nonsurgical retreatment, and apical microsurgery.
Outcomes studies may report success or survival. Survival is the broader representation and refers to the absolute presence or absence of the tooth in the mouth, whether or not there are signs or symptoms of disease. In the prognosis literature, survival is synonymous with “clinically functional.” Success takes that cohort of survived teeth and excludes any with symptoms or radiographic pathology.1 Failure in both includes teeth that have undergone extraction following endodontic treatment.
As far as the numbers are concerned, endodontic procedures are immensely predictable. For nonsurgical root canal therapy, success rates approach 90%; for retreatment, 82%; and for apical microsurgery, 90%.1-3 That said, these reported success rates do not represent absolute numbers. Clinicians should recognize that certain preoperative and treatment-related factors can significantly influence success in endodontics, both positively and negatively.
They must consider these factors, and discuss them with patients, to ensure thoroughness in informed consent. In this article, we focus on outcomes as a means to aid practitioners in treatment planning for endodontics procedures, specifically on how clinical prognostic factors can affect outcomes for the big 3 endodontic procedures. Applying these principles will allow for discussions on expected success and survival tailored to the individual patient.
Prognostic Factors
Patients may present with certain preoperative factors that can directly affect outcomes. Though outside of clinician control, these factors must be considered with respect to treatment planning. The 3 associated with outcome alterations include apical periodontitis, periodontal status, and treatment history. Treatment-related factors go beyond the delivery of competent care. Successful nonsurgical treatment requires the locating, cleaning, shaping, and obturation of the root canal space, whereas surgical treatment requires the resection of the root apex, retropreparation into the root canal space, and adequate restoration of the apex. The treatment-related factors we discuss here represent those items within clinician control beyond the delivery of adequate care and include restorative care and the utilization of modern technologies. The factors are listed in Figure 1, and we discuss each in turn.


Figure 1. Several factors can impact the prognosis following endodontic treatment, including preoperative factors and treatment-related factors. Preoperative factors represent those factors completely outside clinician control, whereas treatment-related factors go beyond the delivery of adequate care.

Apical Periodontitis
A comprehensive endodontic assessment requires a clinical and radiographic examination to formulate both a pulpal and periapical diagnosis. Apical periodontitis, particularly asymptomatic apical periodontitis, represents one of the many periapical diagnoses, and results from the egress of bacteria from a necrotic pulp or previously treated root canal space into the apical periodontium, leading to bony destruction.4 Essentially, the interplay between bacteria and host immune responses causes bony destruction. The bacterial component can present a significant treatment challenge.
The presence of apical periodontitis, and its relative size, are associated with a reduction in success rates following both nonsurgical root canal therapy and nonsurgical retreatment.1,5 This does not mean that patients with a diagnosis of apical periodontitis should be excluded from endodontic treatment. Rather, they should be informed of the factors beyond clinician control that may negatively influence treatment outcomes. The presence of apical periodontitis warrants mention so that patients can understand its interplay with respect to outcomes, particularly if other comorbidities exist. Larger apical radiolucencies are associated with a greater bioburden and more robust immune response, and consequently more effort is needed on the part of the immune system in order to heal. For this reason, patients should be encouraged to pursue endodontic care when lesions are small, rather than delaying until they enlarge. Figure 2 depicts a case where apical periodontitis was successfully treated.

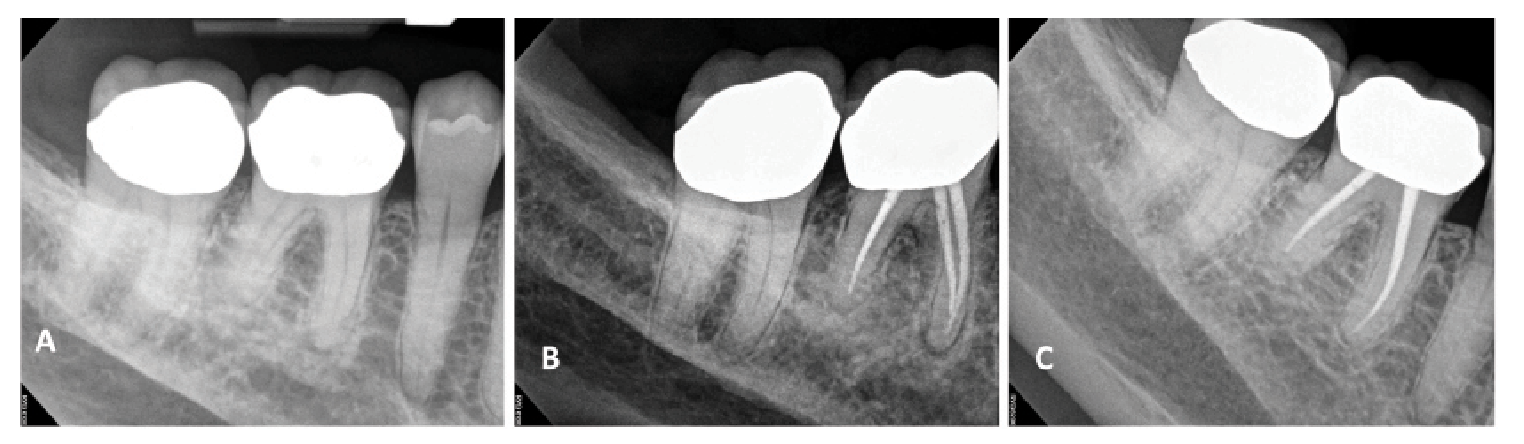
. Endodontic treatment was completed on the tooth (B), and at a 5-year follow-up (C) complete lesion healing was noted.")
Figure 2. Though cases presenting with preoperative apical periodontitis may have a reduced prognosis, complete apical healing is possible following endodontics. This patient presented with preoperative asymptomatic apical periodontitis on tooth #30 (A). Endodontic treatment was completed on the tooth (B), and at a 5-year follow-up (C) complete lesion healing was noted.
Periodontal Attachment Loss
As part of the comprehensive endodontic assessment, a periodontal exam should be performed on endodontic patients, specifically measuring for probing depths and mobility. Marginal periodontitis, like its apical cousin, represents a bony response to bacterial challenges.6 For all the big 3 endodontic procedures, comorbid periodontal disease has the potential to negatively affect treatment outcomes.7 The presence of preoperative periodontal disease increases the odds of tooth loss following nonsurgical root canal therapy more than 5-fold.8 Periodontally involved teeth are similarly lost at higher rates following apical surgery.9 As with apical periodontitis, the presence of periodontal disease does not preclude endodontic therapy as a treatment option for patients; rather, patients must be informed of its potential negative impact on expected outcomes. More severe periodontal disease is associated with a greater likelihood of tooth loss.10 This represents a rationale for early treatment of periodontal disease to prevent progression.
Endodontic Treatment History
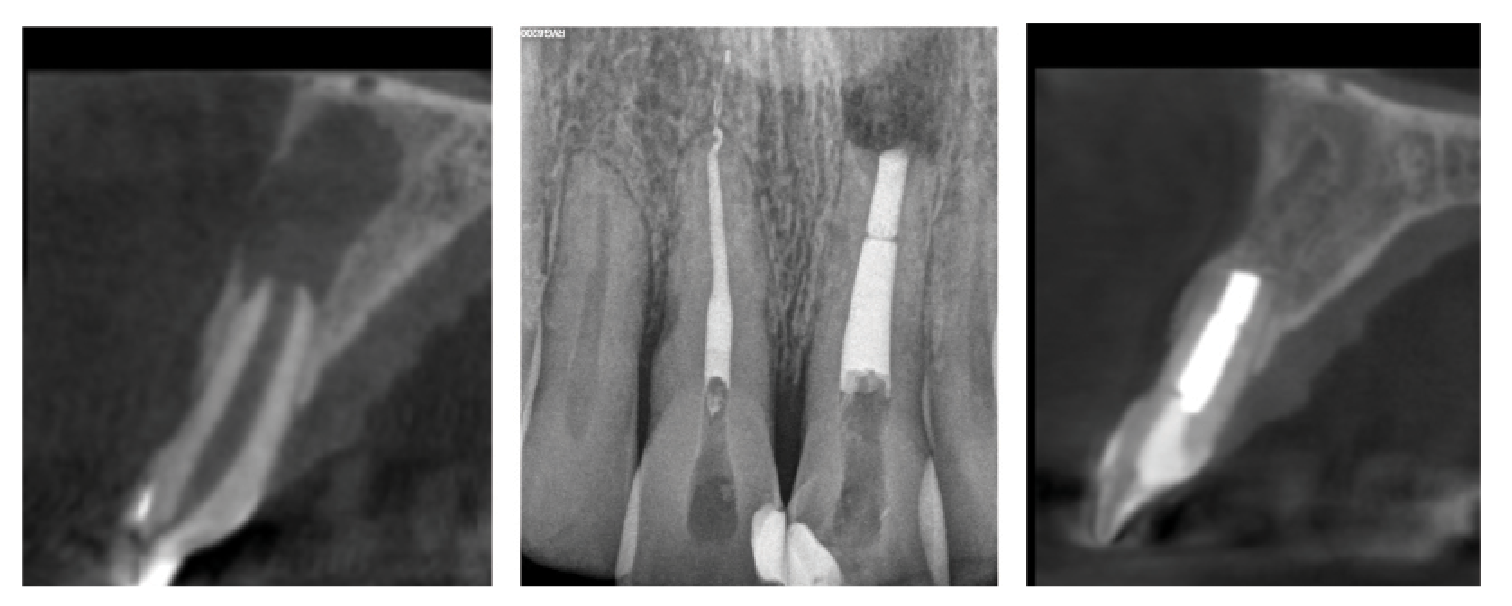
Teeth with a history of endodontic care warrant careful radiographic examination when clinicians are considering nonsurgical and surgical endodontic retreatment. Clinicians must take into account the impact the quality of prior treatment may have on outcomes. Outcomes are more predictable for teeth in which the quality of the initial treatment was poor.2 Poor quality may refer to untreated anatomy, ledged canals, and short fills, among other deficiencies. Clinicians should inform patients that when defined problems are found that can be fixed, outcomes are significantly improved. Quality should also include an assessment of complications from the prior procedure. Outcomes are less predictable for teeth with preexisting complications, including perforations, as seen in Figure 3.5

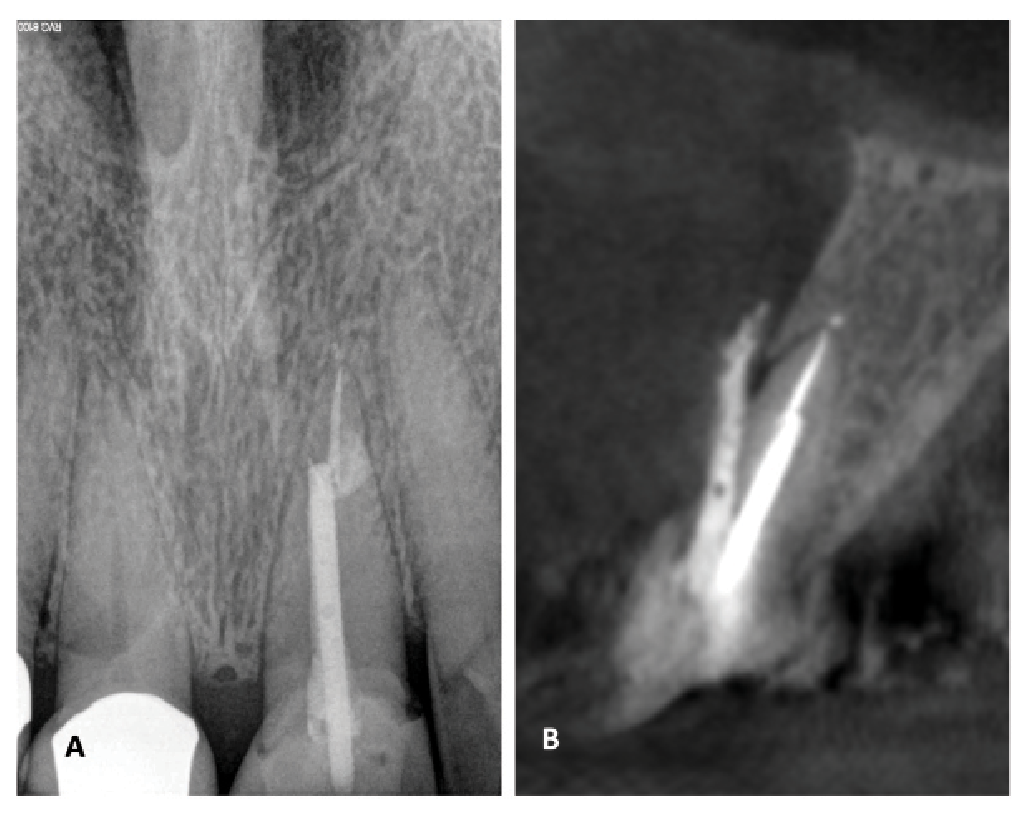
 appeared largely normal, the sagittal view on cone beam computed tomography (CBCT; B) revealed restorative material extruded through a perforation. Extraction was recommended.")
Figure 3. Teeth with preexisting perforations have a poor expected prognosis for nonsurgical or surgical retreatment. This patient presented with severe palpation tenderness and an associated 7-mm periodontal probing depth on the facial aspect of tooth #8. Although the periapical radiograph (A) appeared largely normal, the sagittal view on cone beam computed tomography (CBCT; B) revealed restorative material extruded through a perforation. Extraction was recommended.
Treatment history becomes particularly important with respect to surgical care. When performing surgery on previously endodontically treated teeth, clinicians can expect the outcomes to be far more predictable when the initial treatment quality was poor, particularly with respect to the length of the initial endodontic fill.9 Another historic factor of importance is the technology associated with prior apical surgery. Historically, resurgery involving older surgical techniques using bur retropreparations and amalgam, intermediate restorative material (IRM), or SuperEBA (ethoxy benzoic acid) retrofills was associated with a poor prognosis.3 With more modern surgical techniques, a surgical history may be less relevant in terms of prognosis. Now resurgery is as predictable as initial treatment.11
Restorative Care
The clinician will assess the restorative history and existing coronal structure of any tooth being considered for endodontic treatment. Endodontic care does not exist in a vacuum. Outcomes are intimately tied to restorative care, and consideration with respect to restorability should be given both pre- and postoperatively. Restorability—namely the presence of adequate coronal structure—is perhaps the greatest preoperative consideration in deciding to pursue root canal therapy. Other factors excluded, the ability to maintain a ferrule and cavity wall length has a direct impact on outcomes.12 The same is true for nonsurgical retreatment. Teeth retaining less than 30% of their initial coronal structural volume have a higher proportion of unfavorable outcomes.13
Before delivering endodontic care, clinicians should make patients aware of the importance of definitive restorative care. Teeth that are not definitively restored following endodontic treatment are more than 5 times likelier to undergo extraction.14 The type, quality, and timing of restoration selected all matter with respect to the prognosis for endodontically treated teeth. Outcomes in the posterior dentition are more predictable, with indirect restorations providing cuspal coverage as opposed to direct composites or amalgams, whereas anterior teeth may be successful when restored directly.15
The goals of any coronal restoration, direct or indirect, are to maintain functionality of the tooth, protect the remaining tooth structure, and seal against coronal leakage. Therefore marginal integrity is paramount to positive outcomes following treatment.16 Ideally, definitive restorative treatment should be completed immediately following root canal therapy due to the risks of coronal leakage with temporary restorations and fracture prior to cuspal coverage in the posterior dentition. In one study, patients who delayed definitive restorative care more than 4 months following endodontic treatment experienced a 3-fold higher risk of extraction than those with teeth restored in a timelier manner.17 Ultimately, timely delivery of restorative care can prevent premature loss of endodontically treated teeth.


The PreXion3D Explorer PRO CBCT Scanner is designed to combine precise 3D imaging, large image detail, diagnostics, and digital planning.

Technology
Although many of the preoperative factors we have previously discussed are largely outside clinician control, treatment-related factors, particularly the application of modern dental technologies, give clinicians a direct opportunity to improve patient outcomes. One of the simplest technologies available to practitioners is the dental dam. The bacterial origins of apical periodontitis are directly inhibited by dental dam isolation, which serves to minimize contamination of the root canal system by indigenous oral bacteria. As a result, dental dam isolation is directly associated with improved survival in both initial root canal therapy and nonsurgical retreatment.18,19 The dental dam offers other benefits, such as aiding in visualization by providing a clean operating field and preventing the ingestion or aspiration of dental materials, irrigant solutions, and instruments; thus, its use is considered the standard of care in nonsurgical endodontics.


Surgical microscopes like the PromiseVision 3D from Seiler Instruments provide unprecedented depth of field and field of view.

Magnification—specifically the use of a surgical operating microscope with the added benefit of illumination—represents another means to improve outcomes in both nonsurgical and surgical endodontics. In a retrospective, case-control study, outcomes in teeth treated without magnification were poorer than in those treated with magnification, as apical periodontitis was found more frequently in the former group.20 Stated differently, teeth treated without the use of microscopes developed recurrent pathology (ie, failed) more frequently than teeth treated using high-power magnification and illumination. Intuitively, this makes sense. Successful endodontic therapy is predicated upon finding, cleaning, and filling the entirety of the root canal space. Magnification enhances our ability to find anatomy and therefore our ability to clean it completely. The use of this technology is also associated with improved outcomes for retreatment and surgical endodontics.9,21
CBCT imaging represents a significant development in dental radiography. In 2 dimensions, structural overlap can significantly impede clinicians’ ability to discern the presence, and sometimes absence, of pathology. CBCT imaging facilitates the appreciation of the entirety of the root structure, supporting periodontium, and pulp anatomy, which can aid in the diagnosis of endodontic pathologies, even in the earliest stages.22

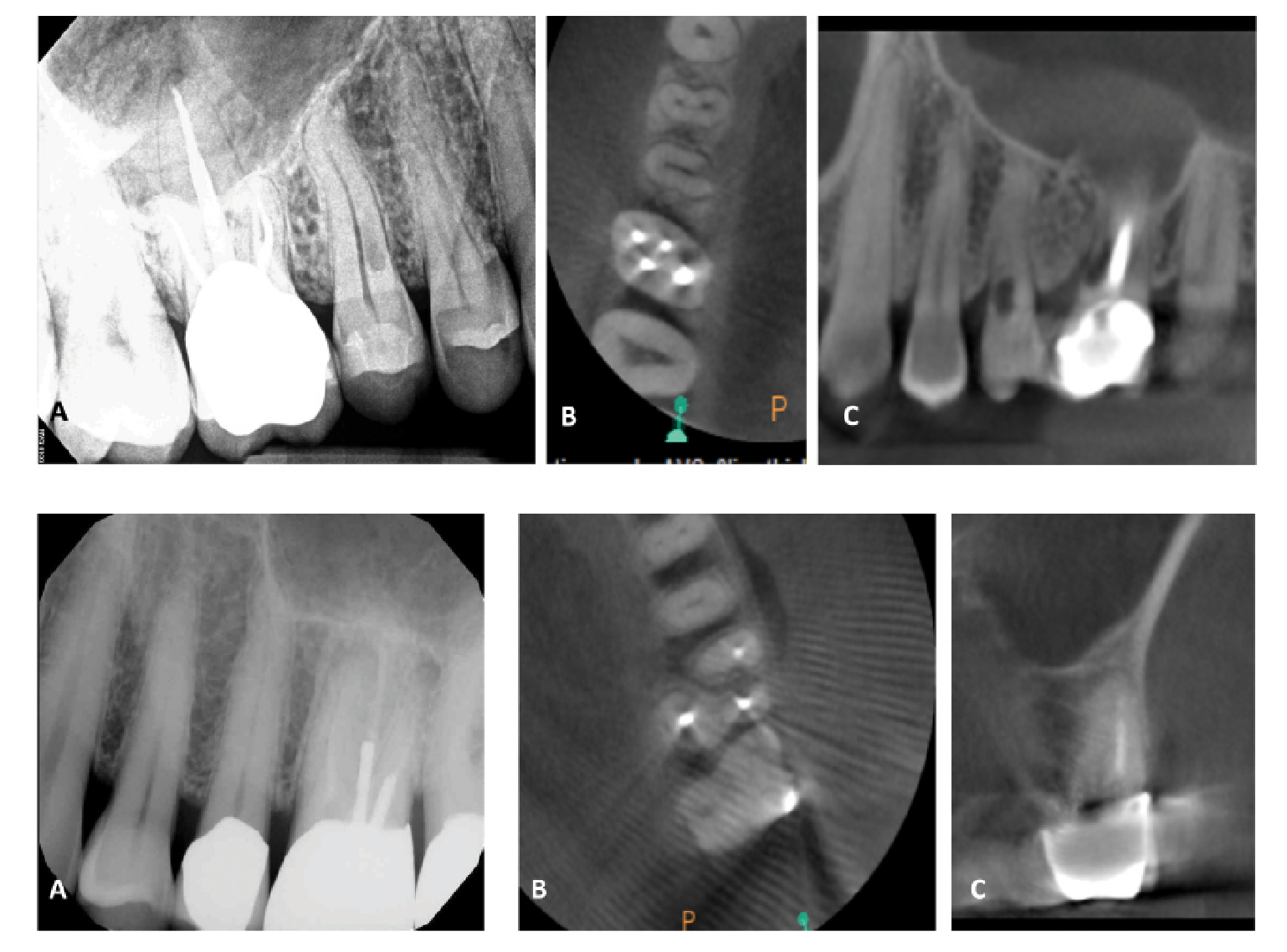
. This patient presented for an evaluation of tooth #4, and the periapical radiograph (A) revealed a resorptive defect on the tooth. Further examination with CBCT noted the palatal resorptive defect on the axial (B) and sagittal (C) sections, as well as additional resorptive defects on tooth #3 that would have gone undetected without 3D imaging.Figure 5 (bottom). This patient presented with biting pain associated with a previously treated tooth #14. The periapical radiograph (A) revealed thin root fillings in the tooth as well as the presence of posts. The axial (B) and coronal (C) CBCT sections revealed evidence of untreated anatomy within the mesiobuccal root of the tooth. Based on an understanding of prognostic factors, retreatment was recommended to address the untreated canal.")
Figure 4 (top). This patient presented for an evaluation of tooth #4, and the periapical radiograph (A) revealed a resorptive defect on the tooth. Further examination with CBCT noted the palatal resorptive defect on the axial (B) and sagittal (C) sections, as well as additional resorptive defects on tooth #3 that would have gone undetected without 3D imaging.Figure 5 (bottom). This patient presented with biting pain associated with a previously treated tooth #14. The periapical radiograph (A) revealed thin root fillings in the tooth as well as the presence of posts. The axial (B) and coronal (C) CBCT sections revealed evidence of untreated anatomy within the mesiobuccal root of the tooth. Based on an understanding of prognostic factors, retreatment was recommended to address the untreated canal.
CBCT technology is particularly useful in identifying factors that complicate a simple endodontic diagnosis, including resorptive dental defects (Figure 4) and fractures.23 With proper diagnosis, resorptive dental diseases can be predictably managed; however, their misdiagnosis can easily lead to failure of endodontic treatment.24 Though CBCT images do not often elicit fracture lines themselves, they can detect very localized areas of bone loss pathognomonic to this pathology. In particular, CBCT images are adept at detecting the narrow, angular bony defects adjacent to fractures, midroot lateral radiolucencies, and bony defects found on the buccal or lingual surfaces that are not visualizable on traditional 2-dimensional radiography.25 As the extension of fractures onto root structure is associated with a less predictable prognosis for treatment, early detection of these defects can facilitate more thoughtful treatment planning.26
CBCT imaging additionally is critical in the assessment of teeth with a history of endodontic treatment. This imaging modality can inform clinicians of the presence of untreated anatomy, procedural errors, fractures, and other findings that can affect future treatment and the resultant prognosis, as previously discussed. With the aid of CBCT imaging, clinicians can develop thoughtful and informed treatment plans that take into consideration the 3-dimensional radiographic realities. Figure 5 illustrates the use of CBCT in assessing a previously treated tooth.
Ultrasonics represent a significant addition to the endodontic armamentarium. Not only does this technology facilitate more conservative endodontic treatment, its use is associated with significantly improved outcomes. The use of ultrasonics, among other armamentaria, during nonsurgical root canal retreatments notably improves outcomes.26 Its utilization is similarly associated with improved outcomes in surgery. These instruments facilitate more conservative osteotomies and create retropreparations that are deep, parallel, and follow the existing anatomy.27 Taken together, these factors result in more conservative and efficacious treatment that in turn results in improved patient outcomes.

, and both nonsurgical and surgical treatment were recommended and completed (B). At 1-year follow-up, complete reformation of the periodontal ligament was noted on sagittal CBCT section (C).")
Figure 6. Apical microsurgery, using modern technologies including magnification, ultrasonic root preparation, and bioceramic-based root filling materials, has an excellent prognosis. This patient presented with a large lesion associated with tooth #9 on sagittal CBCT section (A), and both nonsurgical and surgical treatment were recommended and completed (B). At 1-year follow-up, complete reformation of the periodontal ligament was noted on sagittal CBCT section (C).
Bioceramic materials represent the final technological advancement associated with improvements in prognosis. These represent a significant development in endodontics, especially when applied to apical microsurgery (Figure 6). Their use as restorative materials in the resected and retroprepared root tip offers a dramatic improvement over previously standard materials, including amalgam, SuperEBA, and IRM, and represents the material of choice for modern surgical endodontics. Bioceramic materials seal exceptionally well, even in the presence of moisture, including blood, and are bioactive. They facilitate the deposition of bone and cementum over the apical seal, both of which facilitate better healing.28 These materials have significantly improved outcomes in apical microsurgery compared with older materials.29
Conclusions
Outcomes matter to clinicians but even more so to patients. Prognostic data are fundamental to case selection and can help both clinicians and patients make educated choices regarding the optimal strategies for individualized care. By treatment planning with the end in mind, clinicians can fully appreciate the variables that may impact outcomes and more appropriately care for their patients. Clinicians must recognize that some prognosis-related factors represent insurmountable hurdles, whereas others are entirely within clinician control. Thoughtful consideration of all these factors will facilitate the delivery of predictable endodontic care, allowing clinicians to maintain their patients’ teeth and their confidence.

















