How to manage shade selection and a patient's needs
How one pediatric dentist uses OMNICHROMA to quickly and confidently place composite.



Besides being a very proud father of five successful young adults, and a grandfather of one adorable grandson, I also feel accomplished in my profession as a pediatric dentist. With more than 40 years in my chosen field, an extremely busy time with family, research, teaching and clinical practice, it’s still surprisingly exciting to see new and better dental materials constantly being developed.
For instance, young dental practitioners enters a practice with substantially more available technology than us “old-timers”. They simply wouldn’t accept an older way of charting, nor should they. However, acceptance of new technology is still a slow process with older practitioners and smaller practices less readily adapting to change.1,2
Fortunately, the adaptation to improved restorative materials is a much simpler transition due to advancements in resin-based composites.3 Advancements include increased ease of polishability, the ability to bulk fill the preparation and fully photo-polymerize due to resin/filler optic synergy, and more recently, universal shade matching resin composites.4-6
Universal shade matching resin-based composites are extremely useful in a pediatric practice providing operative care to younger children and those with special needs on a daily basis. Matching the shade without needing to interrupt a procedure is important in time management, especially when time may be limited by patient cooperation and comfort.
The advent of universal adhesives, not requiring the numerous steps and components that once were necessary, has made dental adhesion less complicated and quicker for the dental practitioner.7 This is, however, a situation that has had a few caveats, with early simplified hydrophilic systems not being as reliable and predictable.8
The newer universal adhesives now are less hydrophilic and less acidic, thus claiming to be more resistant to water resorption and hybrid layer dissolution.9,10 Bonding to the smear layer may still be problematic, even with the new universal self-etching adhesives.11 Some clinicians suggest removal of the smear layer with the total-etch technique may still be advisable, especially with a very short dentin etch time of two to three seconds.12
Case study
A patient presented as a 6-year-old female with a medical history of sensory issues and Mast Cell disease as well as a dental history of moderate to severe apprehension. Of note is in this pediatric population, the author’s patients diagnosed with Mast Cell Activation Syndrome appear to also have neurologic sequela, although this has not yet been well defined in the literature.13
Clinically, the patient presented with large carious occlusal lesions of the second primary molars requiring restoration. After consultation with the responsible legal guardian/parent, behavior was to be managed with video distraction, nitrous oxide analgesia and the Single Tooth Anesthesia System® (STA) from Milestone Scientific.
After application of a 20% benzocaine topical gel into the sulcus of the second primary molar, anesthesia was obtained using STA mode with three percent carbocaine.





Fig. 1 Fig. 2
A #4 rubber dam clamp was atraumatically placed and a nonlatex rubber dam applied (Fig. 1). The preparation was performed with a #330 carbide bur from Tri Hawk with copious water spray to reduce smear layer formation11 (Fig. 2). Deep dentin caries was removed with a #4 round bur and a sharp spoon excavator, removing infected but leaving affected dentin (Fig. 3).


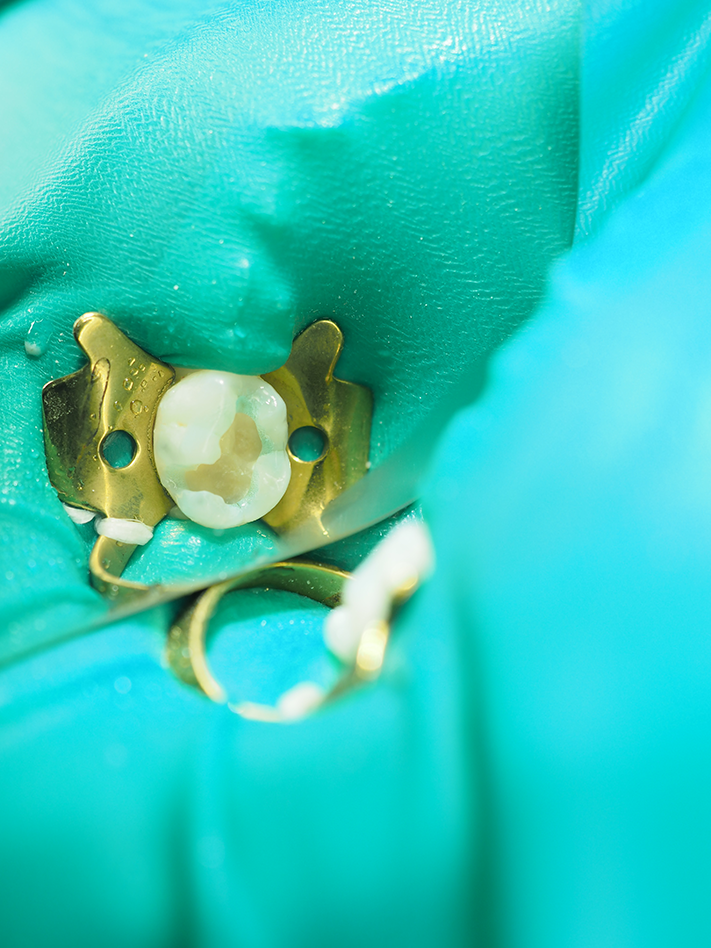
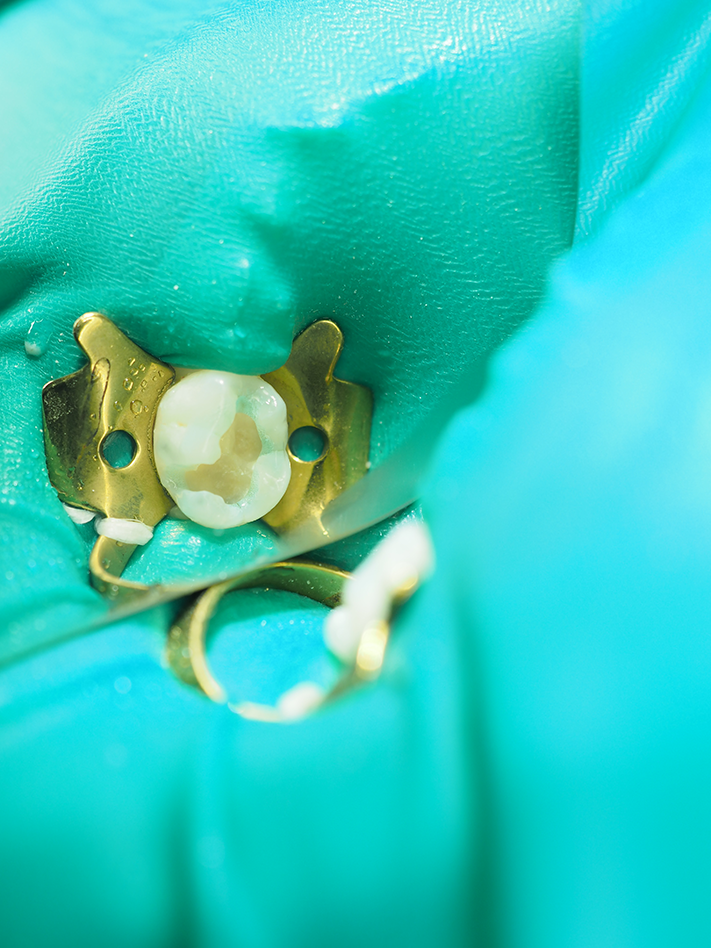
Fig. 3 Fig. 4
Continue to page two to read more...
The preparation was etched with the enamel treated for 30 seconds, and then the etchant was rubbed onto the dentin for two to three seconds to remove the smear layer (Fig. 4). The etchant was then rinsed off for 10-15 seconds, leaving the enamel etched and the smear layer removed but with the dentinal plugs remaining (to reduce sensitivity). A resin-based tricalcium silicate base was then placed and light cured for 20 seconds (Figs. 5 and 6).


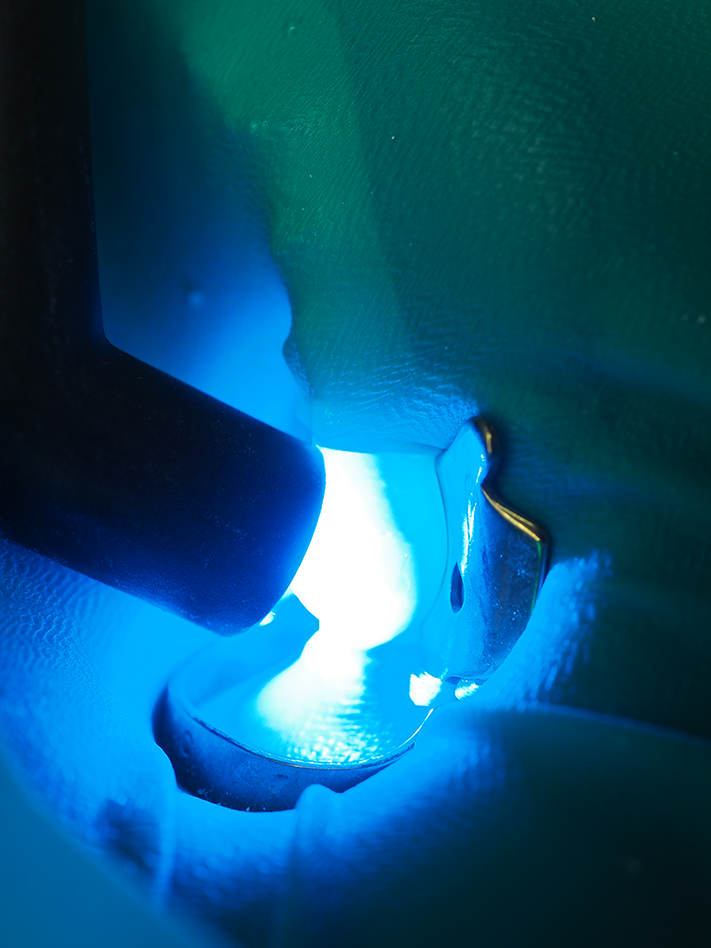
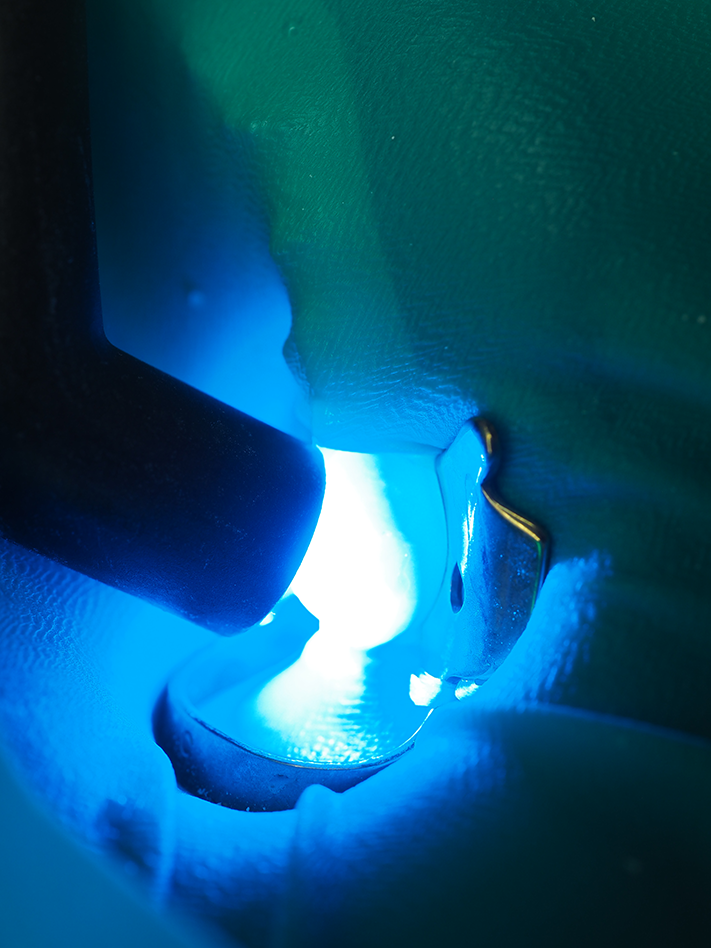
Fig. 5 Fig. 6
Following the light curing, a universal dentin bonding adhesive was gently applied to the preparation and then moderately air dried, taking approximately 25 seconds. Tokuyama Universal Bond from Tokuyama Dental America, an eighth-generation adhesive, is a self-etching adhesive that doesn’t require light polymerization (Figs. 7 and 8).



Fig. 7
OMNICHROMA from Tokuyama Dental America, a universal resin-based composite matches every tooth shade with a single shade of composite, was then incrementally placed in 2 mm layers and light polymerized (Figs. 9 and 10).




Fig. 8 Fig. 9
The final increment had the gross anatomy placed with a lateral condenser, which is also known as an acorn condenser (Fig. 11).




Fig. 10 Fig. 11
Polishing was accomplished with the RAPTOR® bur system from BISCO and Rally rubber points from Garrison Dental. After rubber dam removal, the occlusion was adjusted with a “football”-shaped gold carbide bur, and the restoration was “power cured” to harden the final surface (Figs. 12 and 13).




Fig. 12 Fig. 13
The patient appeared to have a very positive experience, and the parent was quite pleased, both with the child’s behavior and the finished restoration. The patient and parent reported no reaction to the visit nor the materials used.
Providing appropriate restorative care to children and those with special needs is more than just “filling decay.” It’s having the appropriate environment, team members, attitude, training and dental materials that best suit the patient and his or her needs. OMNICHROMA allows the practitioner to confidently place resin-based composites without the added step and time of shade matching. It’s a true benefit for both the young pediatric or special needs patient and the dental practitioner.
References
1. van der Zande, M. M., Gorter, R. C., Aartman, I. H., & Wismeijer, D. (2015). Adoption and use of digital technologies among general dental practitioners in the Netherlands. PloS one, 10(3), e0120725. doi:10.1371/journal.pone.0120725.
2. Milgrom P. M., Horst J.A. The Effect of New Oral Care Technologies on the Need for Dentists in 2040. J Dent Educ. 2017 Aug;81(8):eS126-eS132. doi: 10.21815/JDE.017.019.3. Alexander, G. , Hopcraft, M. , Tyas, M. and Wong, R. (2014), Dentists’ restorative decision making and implications for an ‘amalgamless’ profession. Part 1: a review. Aust Dent J, 59: 408-419. doi:10.1111/adj.12209.
4. Kameyama, A., Nakazawa, T., Haruyama, A., Haruyama, C., Hosaka, M., & Hirai, Y. (2008). Influence of finishing/polishing procedures on the surface texture of two resin composites. The open dentistry journal, 2, 56-60.
5. Van Ende A., De Munck J., Lise D.P., Van Meerbeek B. Bulk-Fill Composites: A Review of the Current Literature. J Adhes Dent. 2017;19(2):95-109. doi: 10.3290/j.jad.a38141.
6. Cannon M. L., Clinical Excellence, Universally Providing the Proper Shade for Posterior Composite Restorations. Dentaltown, March 2019.
7. Trevor Burke F.J., Lawson A., Green D.J.B., Mackenzie L. What’s New in Dentine Bonding?: Universal Adhesives. Dent Update. 2017 Apr;44(4):328-30, 332, 335-8, 340.
8. De Munck J1, Van Meerbeek B, Yoshida Y, Inoue S, Vargas M, Suzuki K, Lambrechts P, Vanherle G. Four-year water degradation of total-etch adhesives bonded to dentin. J Dent Res. 2003 Feb;82(2):136-40.
9. Zhang Z.Y., Tian F.C., Niu L.N., Ochala K, Chen C., Fu B.P., Wang X.Y., Pashley D.H.4, Tay F.R. Defying ageing: An expectation for dentine bonding with universal adhesives? J Dent. 2016 Feb;45:43-52. doi: 10.1016/j.jdent.2015.11.008. Epub 2015 Nov 30.
10. Chen C., Niu L.N., Xie H., Zhang Z.Y., Zhou L.Q., Jiao K., Chen J.H., Pashley D.H., Tay F.R. Bonding of universal adhesives to dentine--Old wine in new bottles? J Dent. 2015 May;43(5):525-36. doi: 10.1016/j.jdent.2015.03.004. Epub 2015 Mar 20.
11. Takamizawa T., Barkmeier W.W., Sai K., Tsujimoto A., Imai A., Erickson R.L., Latta M.A., Miyazaki M. Influence of different smear layers on bond durability of self-etch adhesives. Dent Mater. 2018 Feb;34(2):246-259. doi: 10.1016/j.dental.2017.11.002. Epub 2017 Nov 13.
12. Cannon M. L., How to use cavity liners to provide better care. Dental Products Review. April 2018.
13. Frieri, M. Mast Cell Activation Syndrome. Clinic Rev Allerg Immunol (2018) 54: 353. https://doi.org/10.1007/s12016-015-8487-6.
















