How expanding knowledge brings dentists new powers
The pace and scope of knowledge is increasing, bringing dental professionals new technologies, techniques and ideas.

I'm not sure who came up with the expression "Knowledge is Power" but whoever thought of it was a genius. Those three simple words are true in many different ways. By bringing knowledge into the equation, we become much more powerful in ways we never considered.
Research and development in a myriad of subjects is rapidly increasing the “bottom line” of our knowledge base. Now that we have computers and machine learning, the curve continues to accelerate.
According to Industry Tap Into News, Buckminster Fuller created the Knowledge Doubling Curve. He noticed that until 1900, human knowledge doubled approximately every century. By the end of World War II, knowledge was doubling every 25 years. Today things are not as simple, as different types of knowledge have different rates of growth.
For example, nanotechnology knowledge is doubling every two years and clinical knowledge every 18 months. But on average, human knowledge is doubling every 13 months. According to IBM, the build out of the “internet of things” will lead to the doubling of knowledge every 12 hours. Now, this may seem daunting at first, but if you think about it, having access to all of that knowledge can open doors and let us do things we would never have dreamed of.
In the beginning
It used to be that the general practice was sort of a “clearing house” of sorts for procedures. The GP performed basic restorative procedures and simple procedures such as basic extractions and easy one-canal endodontics. Anything more complicated ended up in the hands of one of the local specialists.
Back then, fluoride was not yet in all the places and substances it is now. Restorative needs of the patients was the “bread and butter” of most general practices. Doctors were so busy restoring large carious lesions they didn’t have the time to learn and implement other procedures into their practices. If the patient’s teeth were misaligned, a referral to the local orthodontist. Impacted third molars? A referral to a local oral surgeon.
As time passed, fluoride began to work its magic and the scope of the general practice began to change. Restorative procedures changed from amalgam and “bombed out teeth” to slot preps and conservative composite procedures, and doctors began to look at ways to expand their services.
The rapid proliferation of internet connections in the late 1990s allowed doctors to connect with other doctors as well as digital databases of research that previously were only available to university or government-based researchers.
This allowed “in the trenches” practitioners to gain access to tremendous amounts of data and leading-edge techniques which allowed them to operate more efficiently and with more predictability. Now a doctor could learn a new technique while eating breakfast and perform the procedure twice before lunch that same day.
This created a feedback loop that greatly changed the way we practice. Whether an online database, an email chain from friends, or one of many other sources of information, the knowledge base of clinical dentistry expanded rapidly.
Sharing
As all of this knowledge expanded, the ability of the general practitioner to treat complicated cases also expanded. Because this expansion of knowledge was stored in a digital format, the ability to share and access that data became a simple matter of “point, click, learn.”
In truth, the doctor had the ability to not only learn, but to then provide immediate feedback to others. This allowed other doctors and educators to quickly evaluate and change procedures so everyone who was “in the loop” could quickly change protocols for the better.
As the operatory computer became the hub of the clinical technology wheel, doctors used their digital integrations to rapidly and reliably share clinical information. Procedures with complications could be tracked and solutions could be advised and attempted in practically real time. Sharing photographs, radiographs and clinical notes with others allowed for the rapid dissemination of clinical information.
Moving forward
We are now entering another phase of our digital practices, one we have been approaching for a decade. Now we are seeing the ability to take the digital data and do more with it!
One of the best examples of this is the data we are aggregating via our intraoral scanners. It used to take several minutes and a certain degree of skill to scan for a single crown. Now full-mouth scans can be accomplished in well under five minutes. This will allow us to take scans at every six-month recare. Why? Because the scanner companies created apps to show how patients’ dentition changes over time. Can you imagine how great a patient education tool that is? I certainly can.
Now let’s look at merging this digital data. Because it is all digital, we can now combine CBCT and digital impression 3D scans. Imagine being able to virtually visualize your treatment inside of a 3D scan before you begin! You can now superimpose your digital impression scans inside your CBCT scans for a constantly updated 3D patient.
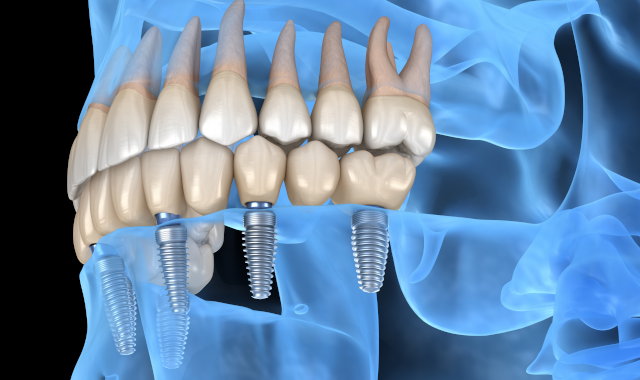
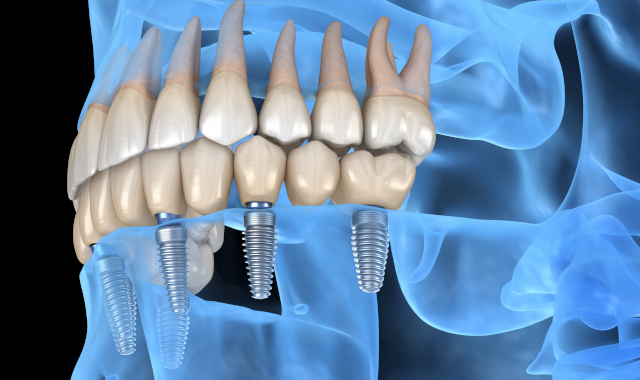
We are already seeing virtual treatment planning for implants which allows a 3D graphical representation of the implant to be placed inside the CBCT volume and then moved via “drag and drop” to the ideal spot for proper support and longevity. Once the implant is “placed virtually,” the file can be sent to a lab where a self- limiting surgical guide is fabricated. The guide is then snapped into the patient’s mouth and the implant is placed with minimal trauma and without a flap. When completed, the implant is in the exact location in which it was placed virtually.
Now let’s take this one step further and simply send the file to the office 3D printer where, in a few hours, the surgical guide is fabricated. We are now able to go from new patient visit to guided implant placement inside of 24 hours.
Or imagine a patient indicating a desire to have straight teeth. You will be able to scan, fabricate the virtual orthodontic treatment plan and print the first aligners. Patients will be able to go from new patient to undergoing clear aligner therapy in less than one business day. Wow!
Diagnosis
Digital data also can be a tremendous aid to the diagnostic process. The fact that diagnostic information is all 1s and 0s means that it can be shared and viewed by anyone we designate anywhere they happen to be. Virtual consults can be simple and easy.
Then there is the matter of using artificial intelligence (AI). There are several groups working on the prospect of AI evaluating radiographs and offering objective second opinions.
In hygiene today, we setup and take radiographs constantly. In the very near future, diagnostic indicators of potential carious lesions will show up in these images automatically. The doctor will “agree” or “disagree” and the system will take that information and learn from it to improve accuracy.
I’ve been experimenting with one of these systems for more than a year and cannot imagine working without it.
Wrapping up
This issue of Dental Products Report is all about “power” and while that term can encompass a lot of different things, power isn’t always about stronger or more resilient or force. Sometimes power can be about knowledge and seeing things from every conceivable angle.
As our skill set progresses further into the digital realm, our profession will work more with virtual diagnosis and treatment planning. We are still going to need incredible hand- eye skills, but we are also going to work with more digital tools. These tools will allow us to create some incredible results for our patients. Dentistry has already done a really great job of setting up digital business and progress notes, but now we are heading into the territory of true digital treatment planning and digital treatment. The future is bright!