Students, employers, and the public have influenced dental schools to incorporate digital dentistry into predoctoral curricula. This study presents graduated dentists’ perceptions of their dental school training in CAD/CAM, application of digital dentistry in practice, and interests in future digital training.
This article is showcasing the research and clinical practice of the faculty and students of Midwestern University College of Dental Medicine and is published in a partnership between the college of Dental Products Report.
623-572-3800
midwestern.edu
An online survey was administered via email to 659 Midwestern University College of Dental Medicine–Arizona (CDMA). Data showed 71.8% of graduates felt “well prepared” to practice CAD/CAM dentistry, and 64.6% of all respondents continue to use CAD/CAM in practice.
The top CAD/CAM digital system in practice was computer-assisted full ceramic dental restoration (66.7% use CEREC). Over a quarter (26.3%) of graduates scanned and sent the restoration to a lab compared with 53.5% who scanned, designed, and milled in-office restorations. Of these, 10.2% of respondents performed CAD/CAM same-day crowns. CAD/CAM crowns (72.7%), onlay/inlays (57.6%), and implant crowns (36.4%) were most popular. More than 60% of respondents saw CAD/CAM as both a time and money saver and a good practice builder. In addition, more than half of respondents from recent years claimed predoctoral preparation in CAD/CAM was a “great advantage” for employment.
Dental schools are hastening to incorporate CAD/CAM and other forms of digital dentistry into predoctoral curricula. It is essential that educators, employers, and manufacturers receive feedback from new practitioners on the utilization of the technologies learned in dental school. According to the study, teaching CAD/CAM benefited most graduates in private, military, and corporate positions. The future of digital dental education is in removable and implant prosthodontics.
Airplanes, the price of gold, and Euclidean geometry directly affected the technology that turned dentistry on its head. In the 1960s, aircraft and automotive engineering companies were experimenting with CAD/CAM.1 By the early 1980s, because of the rise in gold prices,2 a search for metal-free crowns led to the first dental optical scanner. Invented by Dr François Duret and based on Euclidean geometry,3 this scanner captured an image of a tooth and converted it into digital data.4 Dr Werner Mörmann then fabricated the first CEREC, and the rest is dental technological history.
The public’s demand for this state-of-the-art dental care influenced a new paradigm in dentistry.5,6 By the millennium, tens of millions of CAD/CAM restorations had been performed chairside by dentists and in dental laboratories worldwide.1 The traditional, less esthetic porcelain-fused-to-metal (PFM) crowns were replaced with ceramic same-day restorations.1,7 CAD/CAM digital indirect restorations (DIRs) stood the test of time, and research found no significant differences in survival rates between DIR and conventional laboratory-produced services.1,4
Purported as the technology of the future, Anthony Iacopino, DMD, PhD, author of a paper in the Journal of Dental Education regarding new science and dental education, noted that CAD/CAM “went from the domain of the unreliable to mainstream practice.”6
This revolutionary digital dentistry demanded many hours of continuing education for traditional dental practitioners to become the modern clinician-technician. Dentists accepted the new clinical paradigm and the management and maintenance of technical hardware and computer software that went with this new science.6
Private practice trends eventually found their way into predoctoral programs.5 Dental schools, being evidence- and science-based institutions, determined to incorporate CAD/CAM DIR for crowns, onlays, and inlays into curricula, and then digital dental education (DDE) was born.6 DDE is defined as predoctoral education of new technology, including CAD/CAM DIR, CAD/CAM removable prosthetics and orthodontics, cone beam computed tomography (CBCT), hard and soft tissue lasers, and rotary endodontics.5
Per the Commission on Dental Accreditation (CODA), all contemporary dental education programs must regularly assess their use of technology and explore new applications of technological advances to enhance student learning.8 According to Stein et al in a paper on emerging technologies and dental education in the Journal of Dental Education, the most challenging task for new technology inclusion into classrooms and clinics is the “development of new approaches to teaching and learning.”4-7,9
Implementation was found in one study to be best started in preclinical didactic courses in which content could be readily altered.5 Technological inclusion must also address faculty reform.9,10 Also per CODA, faculty development is a necessary condition for change and innovation in dental education.8 Successful implementation has been found with research to lie primarily with faculty and their capacity to individually and collectively interact with students and affect learning.5,10
Other technological inclusion considerations are the physical facilities, cost of operations, effect on student tuition, and class and clinic time allotment.4,5 Additionally, the task of managing cyber-technological infrastructures and learning management systems must be carefully considered.9
Large data repositories and servers are required for electronic data entry, the CAD/CAM computer network, and the milling job servers. Some dental schools could only establish digital centers with limited CAD/CAM technology and student access.4,7,11 With such challenges facing dental schools, younger, smaller institutions were found in early research to be more accepting of incorporating DDE into their curricula.5 These schools were on the leading edge of a new era in dental education.
According to Iacopino, no specific data or studies exist to support the notion that dental graduates and established practitioners are resistant to change and the incorporation of new technologies. It is generally accepted that most new practitioners use the products and technologies they were exposed to and worked with during their dental training.6
As part of the study, after a decade of CAD/CAM dental education, the research team wanted to provide data to either support or deny Iacopino’s statement. The study aimed to gain insights into graduate dentists’ perceptions of their CAD/CAM training in dental school. According to Iacopino, if such training had been successful, the new practitioners would incorporate into dental practice the technology they were taught. Therefore, a survey was designed to ask dental graduates about previous, current, and future practice goals for CAD/CAM technology. The study also sought to gauge graduates’ interests in future DDE and continuing education in digital dentistry (CEDD).
Methods
This research study was approved by the Midwestern University Institutional Review Board (AZ1195). This study’s participants were Midwestern University CDMA graduates between 2012 and 2017.
In 2008, the CDMA opened its doors to its first dental class. The progressive objective of its DDE program was to provide all students with standardized educational experiences and equal access to CAD/CAM technology. In the early stages, admittedly, not all faculty or students had the same clinical experience, comfort, or end results with ceramic technology.
Preclinical simulation labs provided limited experiences in crown preparation, scanning, and milling restorations on manikins with a new digital system called E4D Technologies. E4D’s technology was also selected as the clinical operating system because of its ability for onsite, stackable job milling.4 Two E4D mobile operating carts, milling units, and glazing ovens were available in the clinic. Early intraoral scanning was not always achievable. E4D technology hardware and software had to evolve to provide a predictable end product.
In 2014, Bradford Smith, the new dean at CDMA, committed to growing the CDMA’s CAD/CAM educational experiences for students by increasing access, improving technology, and calibrating faculty. An existing community service program that provided free dentistry to qualified low-income patients was expanded to include CAD/CAM DIR. A Dentsply Sirona CEREC cart delivery system was added to the preclinical simulation lab curricula. Upgraded E4D scanners on multiple mobile carts provided greater access to students in the clinic. Additional full-time clinician faculty with CAD/CAM expertise were also hired. Today, CDMA operates one of the largest E4D (Planmeca) CAD/CAM operations in the United States.
The study used a 23-question mixed-methods survey to assess participants’ perceptions of their dental school CAD/CAM training, CAD/CAM technology in practice, postgraduate CEDD, and the types of DDE to be taught in dental schools in the future. Twenty closed and 2 open-ended questions were created on an online platform in Research Electronic Data Capture (REDCap).12 Three closed-ended questions included demographics and work experiences. One open-ended question queried what digital training or experiences the graduate would have liked to have had in dental school. An open comments section was provided for this question. The questions were self-designed and tested by the authors, who are all practitioners and clinical instructors trained in CAD/CAM technology.
An email inviting participation was sent in August 2018 to 659 graduates. An email reminder was sent 3 weeks later. Data were collected using REDCap electronic data capture tools hosted at Midwestern University. REDCap is a secure, web-based application designed to support data capture for research studies.12
Data was requested from CDMA for PFM, ceramic, and CAD/CAM DIR produced in the clinic from 2014 to 2017. Study data were analyzed by year of graduation for questions on CAD/CAM training in dental school and the possible advantage of CAD/CAM training for employment, as well as whether the respondents were using CAD/CAM technology in practice. Fisher’s exact test was applied to the data on CAD/CAM use in practice. All other data were analyzed as cumulative answers of all respondents.
Results
A total of 99 alumni responded to the survey. Graduates from 2017 comprised 35.7% of respondents, 19.4% were from 2016, and an average response of 11.5% from each of the graduating classes were from 2012 to 2015. There were 57.1% male and 42.9% female respondents, with the majority (82.4%) between ages 24 and 35 and 10.3% between 36 and 40 and 7.2% over 40. Regarding work experience, 25.3% were private practice owners, 48.5% had been or are private practice associates, 40.4% had been or are corporate associates, 15.2% had military experience, 7.1% had been or are in public health, 10.1% had gone into general practice residency programs and advanced education in general dentistry (AEGD), and 7.1% had specialized.
Data results in Table 1 show respondents’ perceptions of preparedness in preclinical and clinical CAD/CAM training, delineated by years of graduation of 2012 to 2017.
Answers ranged from well prepared, minimally prepared, not prepared enough, and no training. Graduates from 2012 (50%) felt not prepared enough in preclinical CAD/CAM compared with 51.4% in 2017 who felt minimally prepared. In clinical DDE, graduates from 2017 (71.4%) and 2016 (42.1%) felt well prepared for private practice. Compared with the classes of 2012 through 2015 who had low responses (8.3%-25.5%) in being well prepared, half of the respondents from 2012 indicated that they had no CAD/CAM training in clinic.
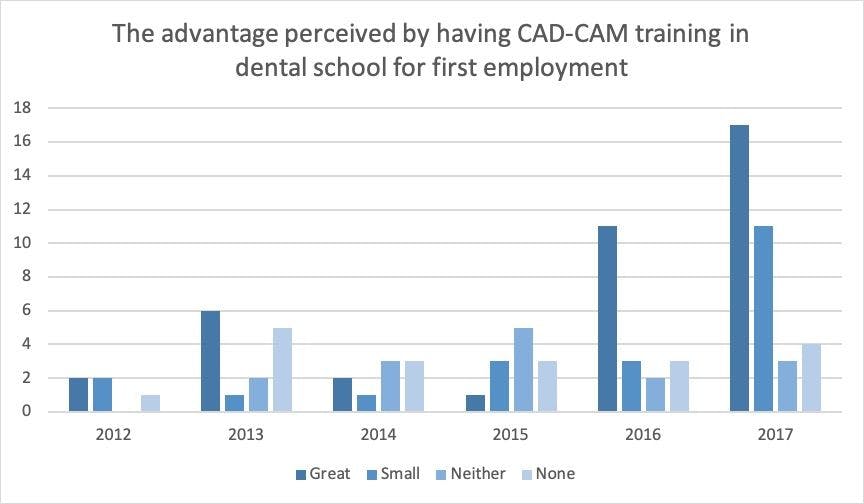
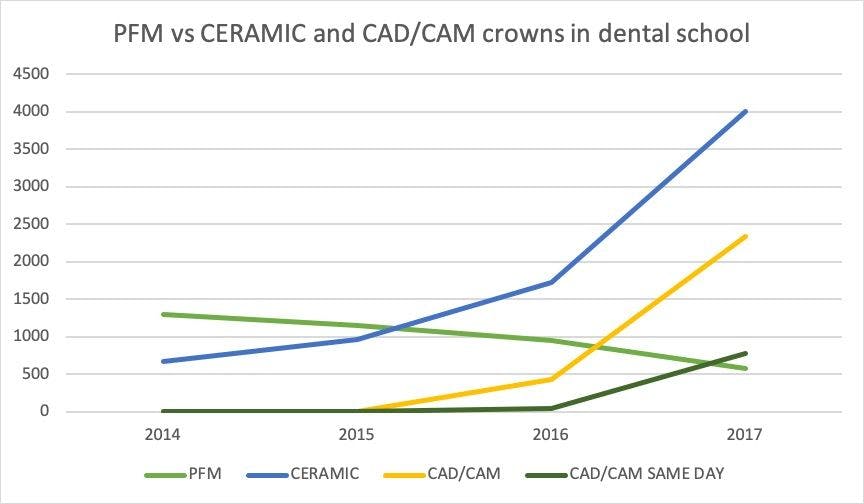
Figure 1 shows that respondents’ perceptions of predoctoral preparation in DDE was an advantage for employment. Years 2016 (57.9%) and 2017 (48.6%) had the highest scores, as DDE predoctoral preparation was a great advantage. A 2016 graduate stated, “The training received in school gave me a leg up on other graduates from dental schools who did not receive such training. It also made picking up CAD/CAM in everyday practice very easy and quick.”
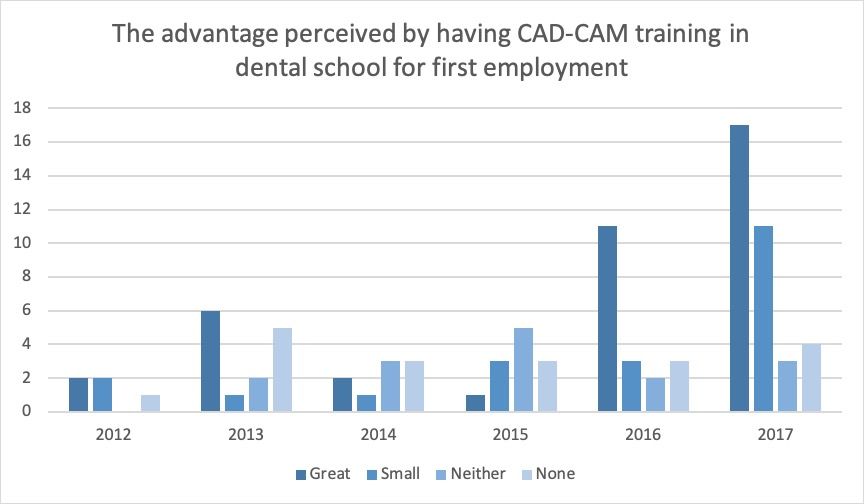
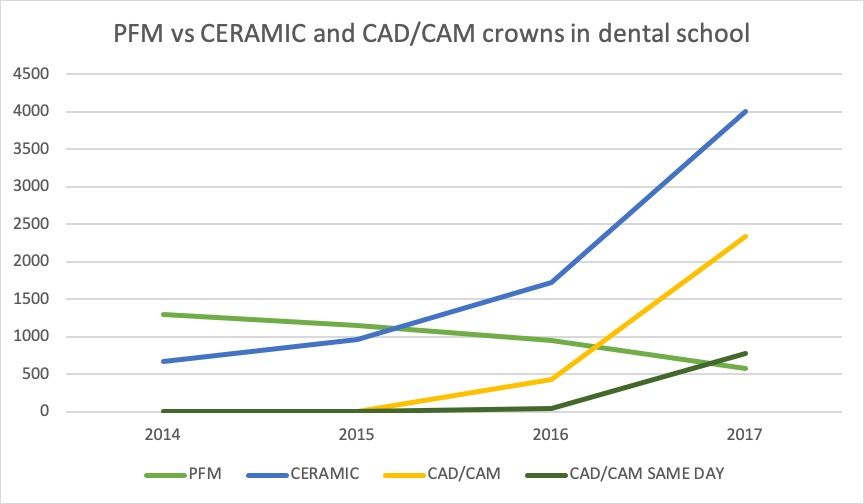
After year 2014, most respondents claimed to have received both preclinical and clinical CAD/CAM training. Figure 2 shows that the number of ceramic DIR grew 4-fold during the period after 2014. In 2017, more than 58% of ceramic restorations were CAD/CAM milled. Same-day CAD/CAM DIR increased from 41 units in 2016 to 780 units in 2017. PFM crown production dropped by more than 50% from 2014 to 2017.
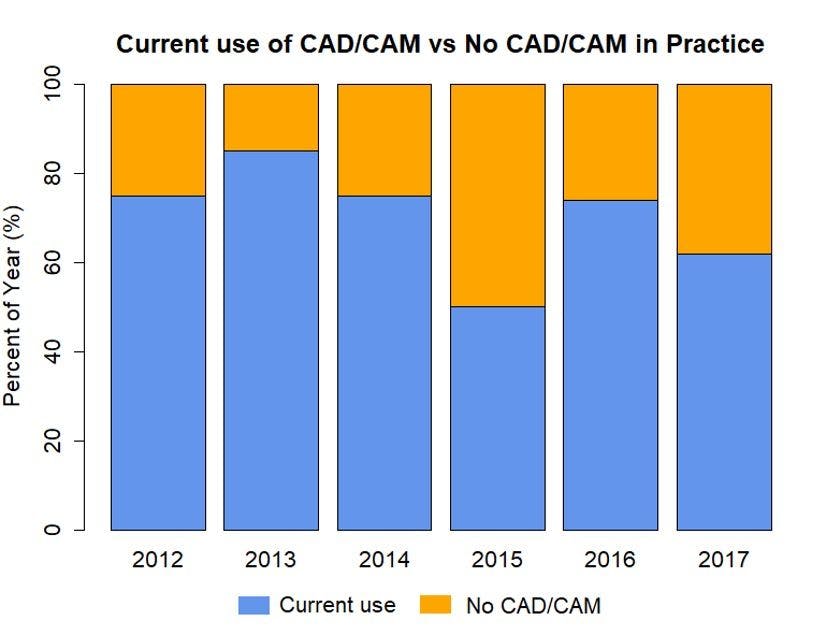
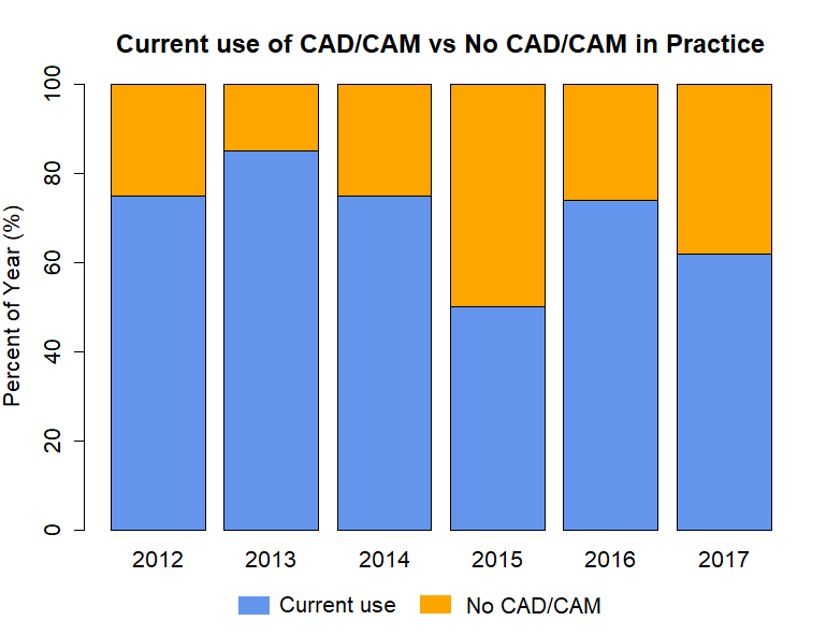
Figure 3 shows, by year of graduation, the number of respondents using CAD/CAM in practice. Fisher’s exact test, on this comparison by year, had a P value of .5302, which showed no significant difference. In addition, 64.6% of total respondents use digital dentistry in practice.
Per the study, the top CAD/CAM digital system in practice was CEREC (66.7%) Over a quarter (26.3%) of graduates have scanned and sent the DIR to a lab. Compare this with 53.5% who scanned, designed, and milled in-office DIR. Of these, 10.2% performed 100% CAD/CAM same-day DIR. CAD/CAM technology, by types of dental procedures, performed by graduates were CAD/CAM crowns (72.7%), onlays/inlays (57.6%), and implant crowns (36.4%) were the most popular. Study data show that although many respondents (61.6%) saw CAD/CAM as both a time and money saver and a practice builder, 47.5% noted that they experienced technical scanner and computer system issues, and 44.4% reported milling concerns.
More than half of the respondents (57.6%) furthered their postgraduate training in CAD/CAM. Hands-on training (88.2%) and in-person lectures (75.0%) for CEDD were most often selected. The CAD/CAM technologies most requested for teaching dental school in the future were implants (83.8%), partial dentures (59.6%), full dentures (65.7%), and orthodontics (53.5%). One-third of the respondents desired training in 3D-printed surgical guides with CBCT integration for implants. The most frequent comment was the desire for greater exposure to other types of scanners and digital systems in dental school.
Discussion
DDE integration into dental schools has been slow in coming,5,7 but CAD/CAM ceramic technology has quickly woven into the fabric of the dental profession. Digital acronyms are the new dental language: CAD/CAM, CBCT, CEREC. Digital dentistry is now so commonplace that it is almost taken for granted.13 Exposure to DDE no longer prepares students for some distant future7; it is to prepare for the reality of dentistry today.
This study’s results show that for DDE to be successful, students must have full access to CAD/CAM technology, digitally experienced and calibrated faculty, and the dental school administration’s full support. Students now demand more from their dental education than just competency and repetition.
Research has shown that after a certain point of learning a skill, additional practice and repetition no longer add further proficiency to that skill.14 Dental schools train in the how of dentistry. Still, millennial students question the why and the what of technology and, according to this study, ask that these be presented in predoctoral programs.15 This study agreed with other research that students expect to receive the “full-digital technique” experience in DDE.16
Research has shown that computer-generated crowns had diminished inaccuracies and allowed practitioners product and artistic control over the restoration.17 CAD/CAM success is well documented, yet few recognize the investment, mechanical, or technical downsides.1-3,17,18 Although named the “most-informed care,”13 CAD/CAM technology was not utilized by new practitioners in this study because of dissatisfaction with the unpredictable and sometimes complex nature of digital technology.
Millennial students are attributed to have been born with an innate adaption to computers and technology.19 They have indeed been born in the age of soaring technological change, but the study agreed with other research that digital exposure does not necessarily equate with digital comfort or proficiency.9 Data from the study showed graduates have mixed perceptions, concerns, and applications of CAD/CAM and digital dentistry.
It appeared that a sector of graduates, either by choice or circumstance, elected to refuse technology. Not all millennial dentists have the budget, the professional opportunities, or the desire for such technology in their practices. Therefore, this study’s results question Iacopino’s assumption that new practitioners will use the technology that they were trained in and worked on within dental school. A graduate cannot predict where they will eventually practice, whether the technology taught to them will be accepted and applied, or whether their circumstance will lead them to resist technological changes. With these unknowns, it is incumbent upon dental educators to provide both conventional dentistry and advanced DDE experiences to all students in preparing them for their careers.
The study found that private, military, and corporate positions highly favored the use of CEREC and CAD/CAM technology. These employment options provided graduates with opportunities to continue applying digital dentistry in their careers. CAD/CAM training also provided advantages in hiring and job placement in certain environments. Graduates in the military noted significant head starts over co-residents in AEGD programs. Others, employed in private and public health dental offices, did not have CAD/CAM technology available and therefore received no advantage from technology training.
The study’s respondents suggested that 3D-printed surgical guides with digital CBCT integration for implants should be taught in dental school.16,20 But technology at that level of complexity may be difficult for many dental schools to achieve. Dentistry and dental schools have always been dependent on practitioners’ obtaining postgraduate lifelong learning. Research has shown that traditional continuing education enhances preexisting knowledge, increases confidence, improves the capacity to use newly learned skills, and helps make evidence-based decisions after graduation.5,10
Dental school training, along with postgraduate CEDD, was projected to blur the line between practice and learning. The 21st-century dental practitioner would integrate both digital education and experience.21 Whether that has been achieved is unknown, but graduates are seeking advanced CEDD to increase their proficiency.
Research has also shown that traditional lecture-based methods in continuing education had short-term benefits and were ineffective in promoting substantial patient care application. In comparison, interactive, hands-on strategies provided greater changes in skills and professional practice.10,22 The study concurred that hands-on experiences for CAD/CAM postgraduate training were the most popular CEDD in the developing fields of orthodontics, implantology, and removal prosthetics.
Although removable complete dentures have been fabricated with CAD/CAM technology since 19943 a recent study noted that CAD/CAM denture fabrication had the lowest acceptance in dental school curricula integration.5 As reported in this study, practitioners are still seeking this removable prosthetics technology. As CAD/CAM digital dentistry continues to improve with 3D printing, prepolymerized materials, and decreased production costs,23 it is projected that dental laboratories, dental students, and the public will demand CAD/CAM dentistry implementation into dental school curricula and CEDD programs.
Previous research assumed that incorporating new technologies into curricula would provide students a greater return on their academic investment.5 Evidenced by the study results that spanned a decade, a program must have ongoing changes and improvements to achieve its DDE goals and provide students with the best academic results for their investment.
Because of student feedback at CDMA, preclinical and clinical faculty rotate every 6 months for greater technology interaction. Clinical student peer pairing adds another layer of local expertise training in technology, such as a third-year student learning from a more experienced fourth-year student.24,25 Ongoing faculty calibration for a common educational vision, diligent customization of computer networks, servers, and CAD/CAM systems should be managed by dedicated clinician-technicians who understand both the dentistry and the technology. Per the study data, dental schools may want to include DDE for troubleshooting and maintenance of the hardware, software, and digital workflow, advancing this clinician-technician concept.
As reflected in the study data, the updates and changes in DDE made by CDMA after 2014 led to significant improvements in student preparedness, consistent learning environments,5 and greater satisfaction and proficiency with CAD/CAM DIR. In 2018, a third-year student was expected to have more than adequate preclinical preparedness in CAD/CAM procedures on their first day of clinic. Students are expected to be able to perform intraoral scanning and strive for same-day CAD/CAM services.
The student has available the latest Emerald scanners from Planmeca, a dedicated milling lab facility, and multiple portable laptops for Planmeca designing. In addition, a zirconia crown digital file can be sent to an in-house lab for processing. The next step in DDE at CDMA is the Ivoclar PM7 prosthetic mill. This mill, along with a 3D printer, was poised to include prosthetic digital technology into the clinical curricula by 2019.
Looking back to how far the profession has come, premillennial dentistry seems archaic. Looking forward, the future of dentistry is a dizzying revolution in 3-dimensional potential.20 Before implementing digital education, an institution may benefit from the outcomes of this study regarding student perceptions of DDE, faculty, curricula, and facility preparation, as well as graduates’ expectations of CAD/CAM technology.21
This study was attempted in comparison with other dental schools that had similar CAD/CAM history and experiences. In the end, a comparison was not achieved, and there were few comparable that have yet to incorporate DDE fully into education.
Further research is warranted to examine how dental schools will continue to incorporate DDE and CAD/CAM removable prosthodontics. One limitation of this study is the respondents may have had recall bias regarding their experiences and perceptions. Because this study took place at a single dental school, the results may not be generalizable to students who have graduated from other dental school programs.
Conclusion
Look back to learn, look forward to succeed; wise words that may apply to educating dental practitioners in CAD/CAM technology. New science inclusion and digital dental education are daunting, evolutionary processes that have both growing pains and great rewards. It is essential that dental educators receive feedback from new practitioners on the utilization of the technologies they were taught to use.
According to the study, teaching CAD/CAM benefited most graduates in private, military, and corporate positions in which digital dentistry is most currently utilized. The challenge for digital dental education is not only the integration of today’s technology into curricula but also all the technology of the future.
References
1. Davidowitz G, Kotick PG. The use of CAD/CAM in dentistry. Dent Clin North Am. 2011;55(3):559-570, ix. doi:10.1016/j.cden.2011.02.011
2. Zarina R, Jaini JL, Raj RS. Evolution of the software and hardware in CAD/CAM systems used in dentistry. Int J Prev Clin Dent Res. 2017;4(4):284-291. doi:10.5005/jp-journals-10052-0127
3. bin Irfan U, Aslam K, Nadim R. A review on CAD/CAM in dentistry. J Pak Dent Assoc. 2015;24(3):112116.
4. Reifeis PE, Kirkup ML, Willis LH, Browning WD. Introducing CAD/CAM into a predoctoral dental curriculum: a case study. J Dent Educ. 2014;78(10):1432-1441.
5. Brownstein SA, Murad A, Hunt RJ. Implementation of new technologies in U.S. dental school curricula. J Dent Educ. 2015;79(3):259-264.
6. Iacopino AM. The influence of “new science” on dental education: current concepts, trends, and models for the future. J Dent Educ. 2007;71(4):450-462.
7. Afshari FS, Sukotjo C, Alfaro MF, et al. Integration of digital dentistry into a predoctoral implant program: program description, rationale, and utilization trends. J Dent Educ. 2017;81(8):986-994. doi:10.21815/JDE.017.050
8. Commission on Dental Accreditation. Accreditation standards for dental education programs. American Dental Association. 2016. http://www.ada.org/~/media/CODA/Files/predoc.ashx
9. Stein CD, Eisenberg ES, O’Donnell JA, Spallek H. What dental educators need to understand about emerging technologies to incorporate them effectively into the educational process. J Dent Educ. 2014;78(4):520-529.
10. Hendricson WD, Anderson E, Andrieu SC, et al. Does faculty development enhance teaching effectiveness? J Dent Educ. 2007;71(12):1513-1533.
11. Browning WD, Reifeis P, Willis L, Kirkup ML. Including CAD/CAM dentistry in a dental school curriculum. J Indiana Dent Assoc. 2013;92(4):40-45,47.
12. Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. doi:10.1016/j.jbi.2008.08.010
13. Hancocks S. What is digital about dentistry? Br Dent J. 2017;223(5):305. doi:10.1038/sj.bdj.2017.732
14. Chambers D. Learning curves: what do dental students learn from repeated practice of clinical procedures? J Dent Educ. 2012;76(3):291-302.
15. Weinstein PK, Wink DM. Beyond Google Docs. Nurse Educ. 2012;37(2):45-47. doi:10.1097/NNE.0b013e3182461c2f
16. Mangano F, Shibli JA, Fortin T. Digital dentistry: new materials and techniques. Int J Dent. 2016;2016:5261247. doi:10.1155/2016/5261247
17. Trost L, Stines S, Burt L. Making informed decisions about incorporating a CAD/CAM system into dental practice. J Am Dent Assoc. 2006;137(suppl):32S-36S. doi:10.14219/jada.archive.2006.0399
18. Rekow ED. Dental CAD/CAM systems: a 20-year success story. J Am Dent Assoc. 2006;137(suppl):5S-6S.doi:10.14219/jada.archive.2006.0396
19. Behar-Horenstein LS, Horvath Z. Generational learning differences in today’s dental students: a popular myth. J Dent Educ. 2016;80(5):588-594.
20. Mangano Guest Editor F. Digital dentistry: the revolution has begun. Open Dent J. 2018;12:59-60. doi:10.2174/1874210601812010059
21. Schleyer TK. Digital dentistry in the computer age. J Am Dent Assoc. 1999;130(12):1713-1720. doi:10.14219/jada.archive.1999.0127
22. Haynes RB, Davis DA, McKibbon A, Tugwell P. A critical appraisal of the efficacy of continuing medical education. JAMA. 1984;251(1):61-64.
23. Srinivasan M, Gjengedal H, Cattani-Lorente M, et al. CAD/CAM milled complete removable dental prostheses: an in vitro evaluation of biocompatibility, mechanical properties, and surface roughness. Dent Mater J. 2018;37(4):526-533. doi:10.4012/dmj.2017-207
24. Mills DA, Hammer CL, Murad A. Power of peers: students’ perceptions of pairing in clinical dental education. J Dent Educ. 2017;81(1):36-43.
25. Roberts EP, Mills DA, Stein AF. Dentist’s perceptions of their peer learning experiences in dental school and effects on practice. J Dent Educ. 2018;83(11):1185-1193. doi:10.21815/JDE.018.123