How to: Treat the Young Adolescent Dental Patient and Prevent Post-operative Sensitivity
Relieving sensitivity in younger patients improves outlook for future dental visits.



Many dental practitioners have reported on the prevalence of tooth sensitivity in their patients following placement of composite resin restorations. This has prompted a number of research studies, clinical trials and reviews of the literature searching for an answer to this common dental issue.1-4
Unfortunately for the dental profession, one out of eight patients already claim they have sensitive teeth before the added insult of dental caries and subsequent restoration.5 This is particularly true for the young dental patient, providing an additional dilemma in pediatric dentistry.6
The proposed solutions to the numerous cited causes for post-operative sensitivity include the following; slow start polymerization, use of self-etch rather than total-etch of the dentin, bulk-fill or incremental-fill, placement of liners or bases, and use of improved dentin adhesives.7
For the young patient, permanent dentition also poses additional challenges as the pulp chamber is larger and the dentinal tubules more patent.8 A more shallow preparation will be relatively closer to the pulp chamber, most likely increasing the post-operative sensitivity prevalence. The young patient is more likely to report and complain about the sensitivity, as it will be a newer condition for them and older patients may actually expect some tooth sensitivity after dental visits.9
It is a major concern for the empathetic practitioner because the first restorative visits may set the stage for the opinion and fears of that young patient for a very long time. Anecdotally, we all have experienced the frightened dental patient, still recoiling from a “bad experience.” Whether it is historically accurate or not, the patient’s opinion of the visit shapes the future patient’s attitude.
Managing teenagers is never easy-ask any parent-and the dental issues may be significant, with potential lifelong consequences.10-11 Very little has been published on the specific needs of the young adolescent dental patient, especially in regards to social context.12-13
As for common dental issues, the erupting permanent molars are typically protected with pit and fissure sealants, unless the grooves and pits present with early carious involvement.14-15 An additional issue may be poorly developed or hypomineralized enamel, as in the case of molar incisor hypomineralization (M.I.H.), with an occurrence rate of almost 10 percent.16 A complicating factor is that restorations of teeth with M.I.H. have been reported to have a reduced survival outcome and a higher rate of post-operative sensitivity.17-18
Naturally, treatment of young adolescent patients requires the use of esthetic materials, cosmetics being a real concern, and the restoration of the carious and/or of the hypomineralized dentition is most often accomplished with resin-based composite materials.19-20 Therefore, reduction of postoperative sensitivity following resin-based composite restorations is even more paramount in the young adolescent dental patient.
Continue reading on the next page...
Clinical technique
A 14-year-old female with history of previous restorative visits at the referring general dental office and a chief complaint of “painful teeth” postoperative presented at my practice.
Unfortunately, pit and fissure sealants had not been previously placed on the patient’s posterior dentition.

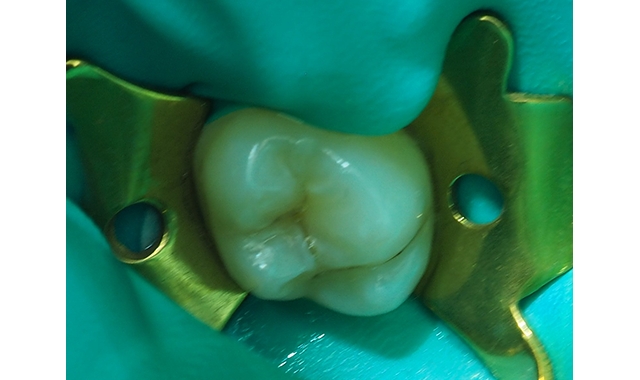
Fig. 1 The pre-operative view, with deep pit caries in newly erupted maxillary second molar.

Consequently, the patient still had carious maxillary second molars to be restored (Fig. 1). She was concerned the restorations would be “painful” postoperatively and worried about the consequences of the planned posterior composite restorations.
To reduce the possibility of another difficult postoperative course, the treatment plan includes a technique using Shield Force Plus from Tokuyama Dental America to reduce postoperative sensitivity after posterior composite restoration.
Following anesthesia from Milestone Scientific’s Single Tooth Anesthesia system using 3 percent Carbocaine with 20,000 Neo-Corbefrin, a rubber dam was carefully placed for tooth isolation. The injection technique was performed with minimum pressure after the placement of topical anesthesia gel, 20 percent benzocaine, into the sulcus. The injection sites were carefully spaced to allow for complete dental anesthesia but not in a manner to increase the possibility of postoperative discomfort.

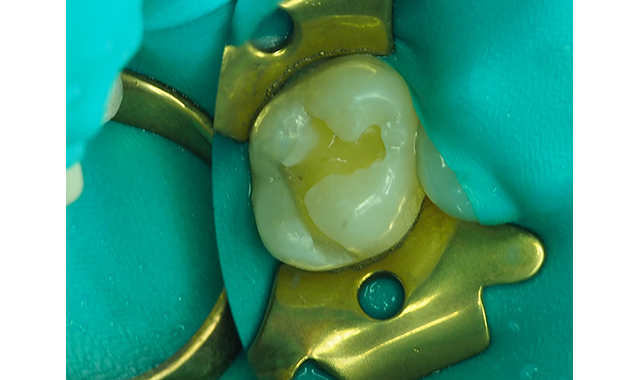
Fig. 2 Rubber dam placed post-anesthesia and the molar prepared with #330 carbide bur in high-speed handpiece with copious water spray.
Continue reading on the next page...
After placement of the rubber dam, the preparation was performed with a high-speed handpiece using sufficient water spray and the carious dentin exposed (Fig. 2). The carious infected dentin was removed with a #4 round bur (keeping the dentin moist) in a slow-speed handpiece and with judicious use of a sharp spoon excavator (Fig. 3).

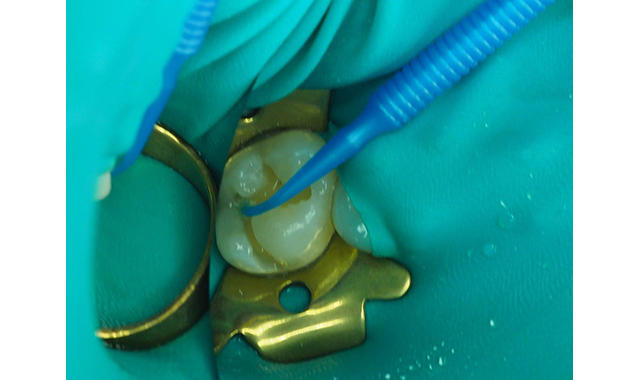
Fig. 3 The carious dentin has been carefully removed with a #4 round bur in a slow-speed handpiece and a sharp spoon excavator. The dentin is never dried and kept moist.
Due to the patient’s history of postoperative sensitivity, a layer of Shield Force Plus desensitizer was carefully applied only to the prepared dentin. Shield Force Plus was allowed to infiltrate the dentin for 10 plus seconds, followed by a stream of light air for 5 seconds, then strong air for five additional seconds, and finally, it was light polymerized for 10 seconds (Figs. 4,5).

Fig. 4 Shield Force Plus is dispensed into a dappen dish. This is done just prior to applying the material to prevent evaporation of solvents.


Fig. 5 The Shield Force Plus applied to the dentin for 10 seconds, slowly air-dried for 5 seconds followed by 5 seconds of strong air drying, and then light-cured for 10 seconds.
Continue reading on the next page...
Due to the history of sensitivity, the judicious placement of etchant only on the enamel, selective etch, was considered. Another viable option would utilize the self-etch technique, also reportedly less likely to cause postoperative sensitivity.4,7
The decision was made to use the self-etch technique utilizing Tokuyama Universal Bond from Tokuyama Dental America, self-cured and self-etched truly universal adhesive. The Tokuyama Universal Bond adhesive Part A and B components were mixed together and then applied to the de-sensitized dentin and cut enamel (Fig. 6). Tokuyama Universal Bond, considered an eight-plus generation adhesive, was dried with gentle air for 5 seconds followed by 5 seconds medium air to evaporate the solvents, while no light curing was required.

Fig. 6 Mixing and application of Tokuyama Universal Bond, which is a self-cure universal adhesive.

Fig. 6 Mixing and application of Tokuyama Universal Bond, which is a self-cure universal adhesive.
The preparation was then filled in increments of less than 4 mm with Estelite Bulk Fill Flow shade A1 from

Fig. 7 Estelite Bulk Fill Flow placed and light polymerized in two increments to restore the molar.
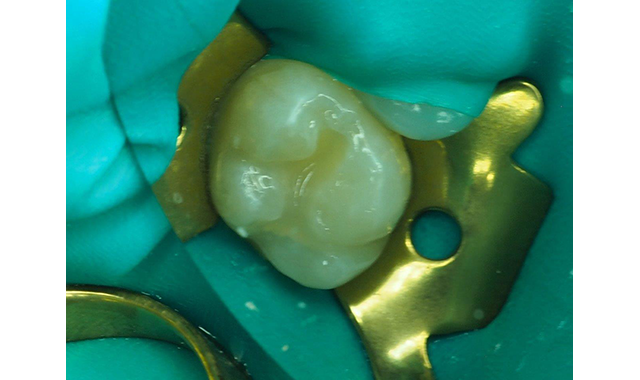

Fig. 8 Light curing of the final increment of Estelite Bulk Fill Flow.
Continue reading on the next page...
Tokuyama Dental America (Figs. 7,8). Following light curing of the final increment of Estelite Bulk Fill Flow, the gross anatomy was achieved with a Raptor bur from BISCO (Fig. 9).

Fig. 9 The gross anatomy was created with the Raptor bur from BISCO.
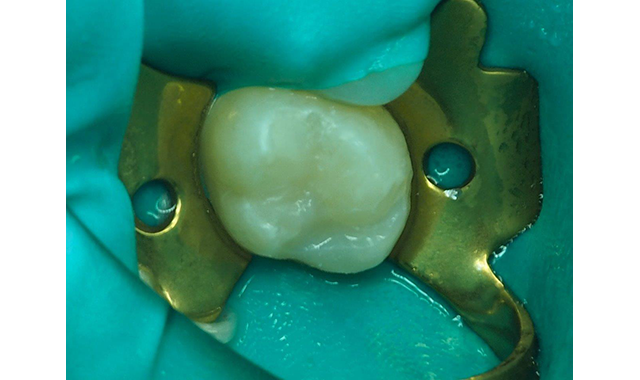
Fig. 9 The gross anatomy was created with the Raptor bur from BISCO.
The rubber dam was then removed, and the occlusion adjusted with a spiral multi-fluted carbide bur followed by fine polishing with Rally points from Garrison Dental Solutions (Fig. 10).

Fig. 10 The occlusion was adjusted and the final polish accomplished with spiral multi-flute carbide bur and polishing points.

The patient’s parents were contacted the next day to check on the postoperative sensitivity and they were pleased to report the patient had none. In this situation, the desensitization of the prepared dentin delivered an exceptional restoration outcome, without post-op sensitivity and improved the dental attitude of this young dental patient.
Creating a happier young dental patient should produce a more ideal end result as they will not be hesitant to seek proper dental care in the future.
References:
- Monu Survashe et al. (2016), Immediate Post-operative Sensitivity after Composite Resin Restoration – A Review of Treatment Protocol. Int J Dent and Oral Heal.2:2, 14-23. DOI: 10.25141/2471-657X-2016-2.0046
- Berkowitz, G., Spielman, H., Matthews, A., Vena, D., Craig, R., Curro, F., & Thompson, V. (2013). Postoperative hypersensitivity and its relationship to preparation variables in Class I resin-based composite restorations: findings from the practitioners engaged in applied research and learning (PEARL) Network. Part 1. Compendium of continuing education in dentistry (Jamesburg, N.J. : 1995), 34(3), e44–e52.
- A. L. F. Briso, S. R. Mestrener, G. Delício, R. H. Sundfeld, A. K. Bedran-Russo, R. S. de Alexandre, and G. M. B. Ambrosano (2007) Clinical Assessment of Postoperative Sensitivity in Posterior Composite Restorations. Operative Dentistry: September 2007, Vol. 32, No. 5, pp. 421-426.
- Costa T.R.F., Rezende M., Sakamoto A., Bittencourt B., Dalzochio P., Loguercio A.D. Reis A. (2017) Influence of Adhesive Type and Placement Technique on Postoperative Sensitivity in Posterior Composite Restorations. Operative Dentistry 42:2, 143-154. Online publication date: 3-Mar-2017.
- Cunha-Cruz, J., Wataha, J. C., Heaton, L. J., Rothen, M., Sobieraj, M., Scott, J., … Northwest Practice-based Research Collaborative in Evidence-based DENTistry (2013). The prevalence of dentin hypersensitivity in general dental practices in the northwest United States. Journal of the American Dental Association (1939), 144(3), 288–296. doi:10.14219/jada.archive.2013.0116
- The Reference Manual of Pediatric Dentistry. American Academy of Pediatric Dentistry 2019.
- Reis A., Dourado Loguercio A., Schroeder M., Luque-Martinez I., Masterson D., Cople Maia L. Does the adhesive strategy influence the postoperative sensitivity in adult patients with posterior resin composite restorations? A systematic review and meta-analysis. Dent Mater. 2015;31(9):1052-1067.
- Sue M., Oda T., Sasaki Y., Ogura I.. Age-related changes in the pulp chamber of maxillary and mandibular molars on cone-beam computed tomography images. Oral Radiol. 2018 Sep;34(3):219-223. doi: 10.1007/s11282-017-0300-1. Epub 2017 Aug 7.
- Ghanei, M., Arnrup, K., & Robertson, A. (2018). Procedural pain in routine dental care for children: a part of the Swedish BITA study. European archives of pediatric dentistry: official journal of the European Academy of Paediatric Dentistry, 19(5), 365–372. doi:10.1007/s40368-018-0368-2
- Cabrera, F., Herrera, A., Rubalcava, S., & Martínez, K. (2017). Behavior Patterns of Antisocial Teenagers Interacting with Parents and Peers: A Longitudinal Study. Frontiers in psychology, 8, 757. doi:10.3389/fpsyg.2017.00757
- Masoe, A. V., Blinkhorn, A. S., Taylor, J., & Blinkhorn, F. A. (2014). Preventive and clinical care provided to adolescents attending public oral health services New South Wales, Australia: a retrospective study. BMC oral health, 14, 142. doi:10.1186/1472-6831-14-142
- Paiva, P. C., de Paiva, H. N., de Oliveira Filho, P. M., Lamounier, J. A., Ferreira e Ferreira, E., Ferreira, R. C., … Zarzar, P. M. (2014). Development and validation of a social capital questionnaire for adolescent students (SCQ-AS). PloS one, 9(8), e103785. doi:10.1371/journal.pone.0103785
- Broadbent, J. M., Thomson, W. M., & Poulton, R. (2006). Oral health beliefs in adolescence and oral health in young adulthood. Journal of dental research, 85(4), 339–343. doi:10.1177/154405910608500411
- Ahovuo-Saloranta, A., Forss, H., Walsh, T., Nordblad, A., Mäkelä, M., & Worthington, H. V. (2017). Pit and fissure sealants for preventing dental decay in permanent teeth. The Cochrane database of systematic reviews, 7(7), CD001830. doi:10.1002/14651858.CD001830.pub5
- Naaman, R., El-Housseiny, A. A., & Alamoudi, N. (2017). The Use of Pit and Fissure Sealants-A Literature Review. Dentistry journal, 5(4), 34. doi:10.3390/dj5040034
- Davenport, M., Welles, A. D., Angelopoulou, M. V., Gonzalez, C., Okunseri, C., Barbeau, L., … Hodgson, B. D. (2019). Prevalence of molar-incisor hypomineralization in Milwaukee, Wisconsin, USA: a pilot study. Clinical, cosmetic and investigational dentistry, 11, 109–117. doi:10.2147/CCIDE.S172736
- Fragelli CM, Souza JF, Jeremias F, Cordeiro Rde C, Santos-Pinto L. Molar incisor hypomineralization (MIH): conservative treatment management to restore affected teeth. Braz Oral Res. 2015;29
- William V, Messer LB, Burrow MF. Molar incisor hypomineralization: review and recommendations for clinical management. Pediatr Dent. 2006;28:224–32.
- Kotsanos N, Kaklamanos EG, Arapostathis K. Treatment management of first permanent molars in children with Molar-Incisor Hypomineralisation. Eur J Paediatr Dent. 2005;6:179–84.
- Opdam, N. J., van de Sande, F. H., Bronkhorst, E., Cenci, M. S., Bottenberg, P., Pallesen, U., … van Dijken, J. W. (2014). Longevity of posterior composite restorations: a systematic review and meta-analysis. Journal of dental research, 93(10), 943–949. doi:10.1177/0022034514544217

















