Technique: Digital case management of a delayed immediate implant placement
How the CS 3600 and CS Connect simplified case planning and execution.

In February 2017, a 68-year-old female presented to my office with a toothache on the lower right side. She stated that the tooth had been hurting sporadically for a week and was worsening in duration and frequency. A review of her medical history showed high blood pressure controlled with medication, but otherwise no medical contraindications.
Upon examination, it was revealed that tooth #30 had large MOD alloy that had fractured with large recurrent decay present. Tooth #29 had previous root canal treatment and a fractured crown; all that remained was the root. After diagnosing the site, I informed the patient of the following treatment options:
Trending article: How to create a better, permanent smile
1. Do nothing, the risks of which could be drifting of adjacent teeth, continuance of the pain and discomfort, further supra-eruption of maxillary teeth and further atrophy of bone, which could make implant placement in the future more difficult.
2. Extract teeth numbers 29 and 30 and restore with a removable partial denture. The patient stated she had no interest in a removable appliance.
3. Extract teeth numbers 29 and 30 then restore site numbers 29 and 30 with a four-unit fixed partial denture (bridge). After discussion with the patient regarding bridge fabrication, she stated she preferred not to involve adjacent teeth.
4. Extract teeth numbers 29 and 30 then restore with single tooth implants. We discussed the different types of implants that are available at this time to restore the site. We also discussed the process of a delayed immediate implant placement as well as bone grafting the extraction sites and returning for the implant placement in approximately three to four months. She was advised that during the procedure the surgeon may deem it more appropriate to abort the placement surgical procedure and graft the site or sites and place the implants at a later visit.
Trending article: How to do same-day implant restoration
The patient was aware of alternative procedures and decided to restore teeth #29 and #30 with single-tooth Bicon Dental Implants. I extracted teeth numbers 29 and 30, and let it heal for two weeks; the patient then returned for a delayed immediate implant placement in the sites.
Next: The treatment plan
Treatment
One week later, the patient returned to my office for her pre-operative visit, during which time her medical history was reviewed and showed no changes. A CBCT scan was obtained with the CS 8100 3D (Carestream Dental) and an implant virtually planned. The pre-op visit gave us another opportunity to discuss the planned treatment, have the patient review and sign her informed consent forms, review the post-operative instructions and electronically prescribe her pre-operative medications.
Related reading: Applying the CS 8100 in your practice

CS 3600

The patient’s next visit was for the delayed implant placement surgery. Manual palpation of the ridge was performed while viewing the 3D scan to confirm the best length and angulation of implants to be used. After review of the CBCT scan, the ultimate length of the osteotomy would be 10 mm from crestal ridge. Bicon Dental implants, 4.5 mm D X 8 mm L mm in site #29 and 6.0 mm D X 8 mm L in site #30, were placed. The patient was followed post-operative one day, one week and two weeks, and sutures were removed after three weeks.
The patient returned after four months for site evaluation. At that time, the tissues were deemed to have healed properly. The implants were uncovered, healing abutments placed and the sites allowed to heal for three weeks. The patient returned and, after removal of the healing abutments, the site had now developed nice emergence profiles.
Related reading: How the CS 3600 intraoral scanner can improve your patient experience
The workflow protocol of the CS 3600 intraoral scanner is such that the full maxillary (opposing) arch was scanned, then the mandibular arch without healing heads for a soft tissue scan. Next, the bite registration scan was obtained. The workflow now calls for a cutting procedure to remove site numbers 29 and 30 from the previous scan; scan bodies were placed and a final scan was performed adding this digital information to the full arch.
Next: The next steps of the case.
The scans were saved in the patient’s chart and sent digitally as .STL files through the CS Connect portal to Bicon Dental Labs and used in the ultimate fabrication of single tooth integrated abutment crowns (IAC).





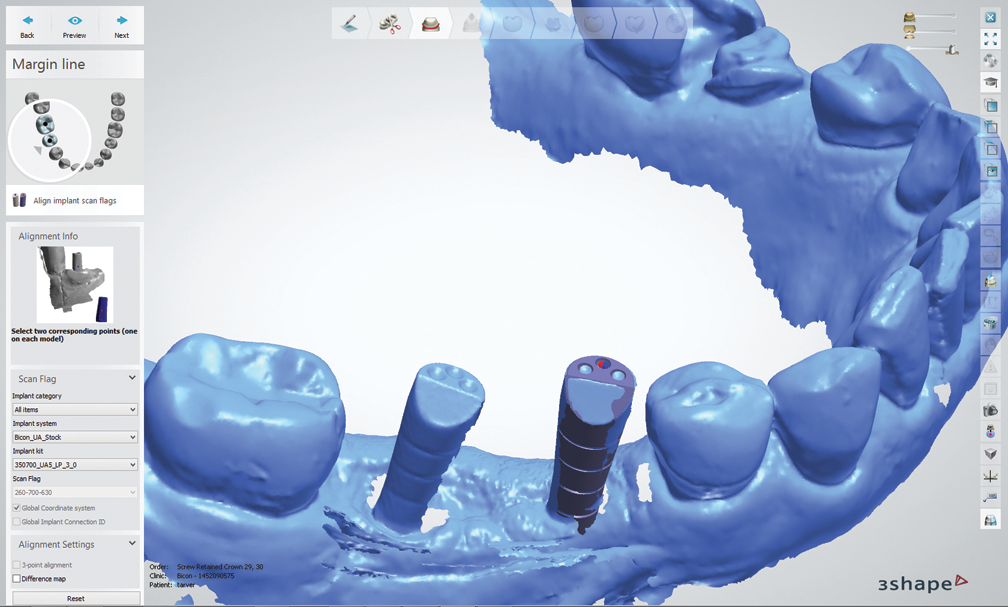
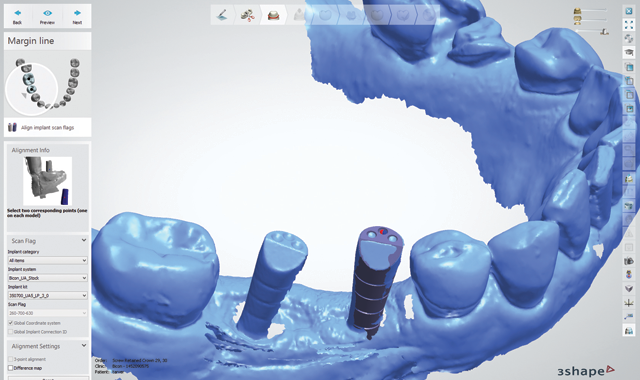
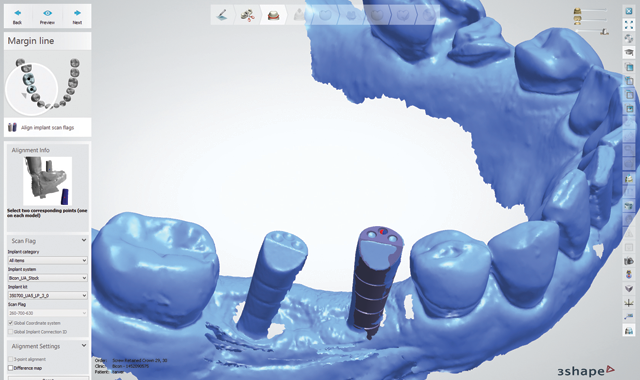
Fig. 1 Fig. 2
Bicon Dental’s digital technician, Joe Cautillo, took the .STL files, utilized 3Shape’s dental design software and communicated with me via email (Figs. 1-7); once he had placed different abutments, I could choose which abutment I preferred for the final implant restoration.


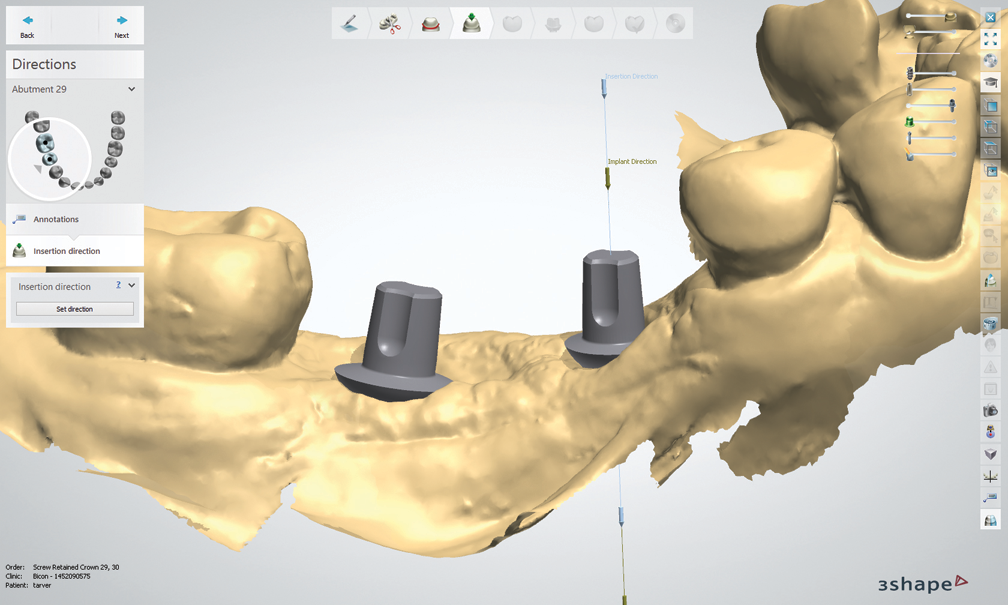


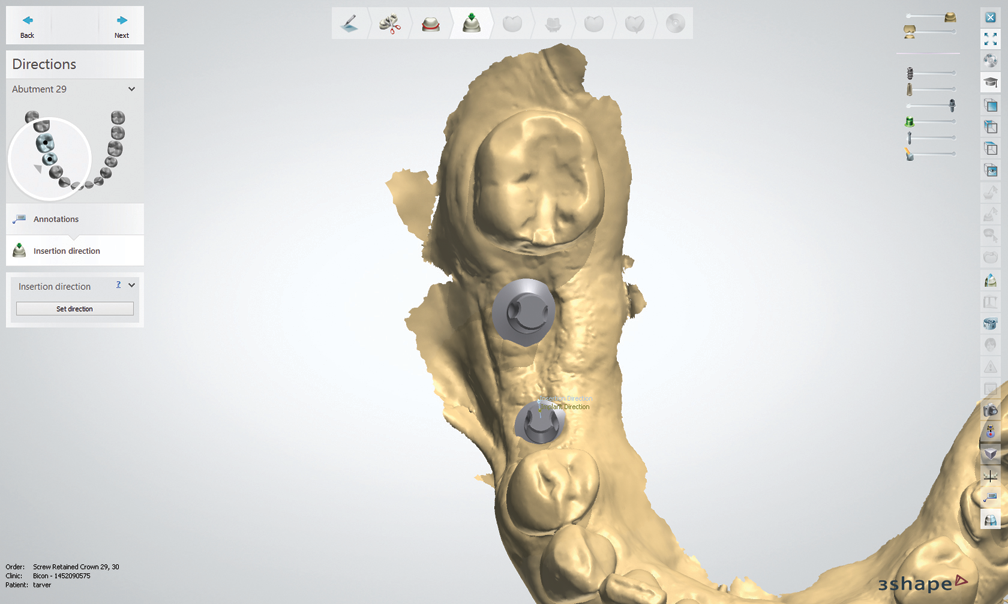
Fig. 3 Fig. 4
After I chose the abutments, Cautillo used 3Shape’s software to design the integrated abutment crowns (IAC) for site numbers 29 and 30. Once they were completed, he sent me an email with the design process to show different views of the crowns and their occlusal schemes.

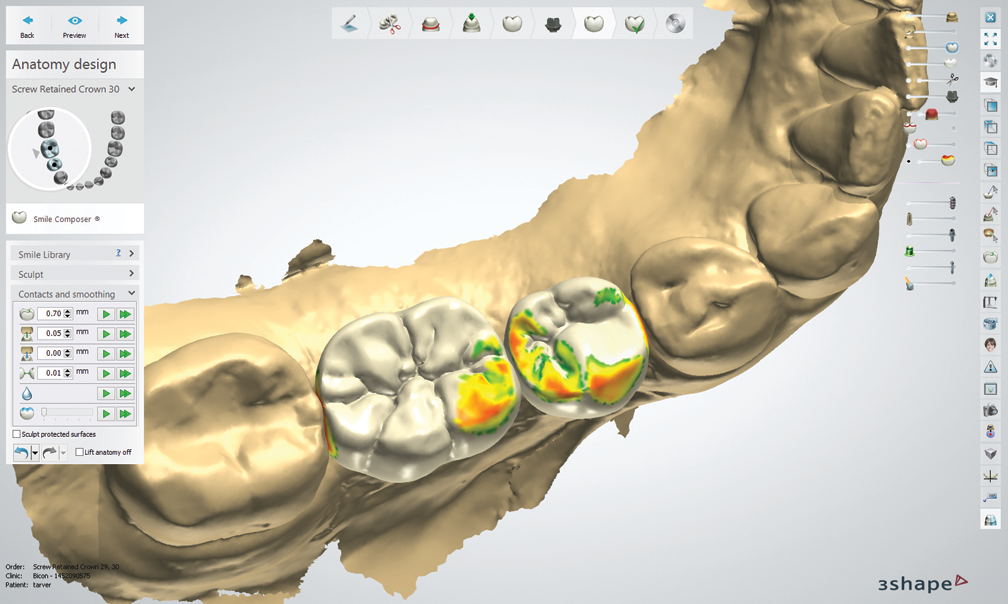

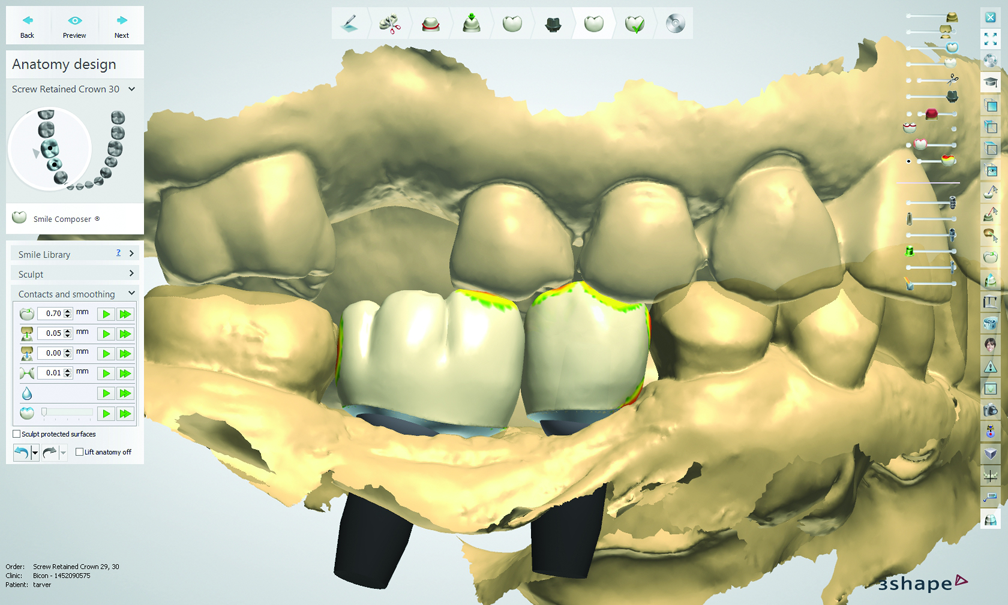
Fig. 5 Fig. 6



Fig. 7
Next: The culmination of the case.
Approximately 2 ½ weeks after sending the files via CS Connect, I received the single-unit integrated abutment crowns from Bicon (Fig. 8). The crowns were tried in with very minimal interproximal or occlusal adjustment (Figs. 9 and 10), and the patient was very happy with the results.


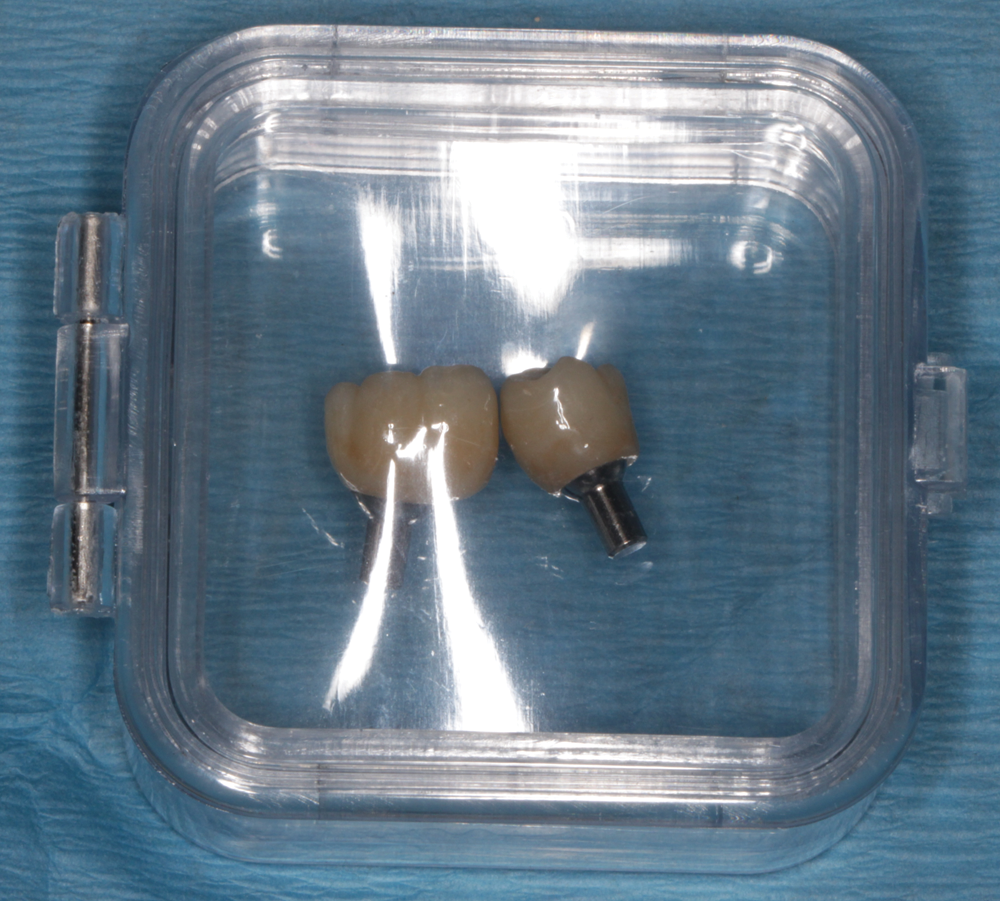



Fig. 8 Fig. 9
In addition to the technology used to treat this patient, I attribute a great deal of the case’s success to the information I have learned from my mentor and coach, Dr. Edward Mills. He has taught me to treat each case individually, utilizing all the diagnostic skills and technology available and suitable for the situation.1



Fig. 10
Digital case management
The CS Connect portal allowed me to easily communicate with the lab. In addition to sending over the .STL files, I was able to upload photographs of the patient (including the teeth, smile lines and contours) in order to help the lab with the design process and shade duplication. CS Connect also allowed me to upload the lab’s prescription form with my comments and desired occlusal scheme for the IACs.
Trending article: Carestream launches two products designed to simplify scanning and imaging
One of the biggest benefits of CS Connect is the speed. As soon as I submit the information, it arrives at the technician’s bench. And the entire process was accomplished without any stock abutment trays, polyvinyl siloxane, shipping charges, boxing of materials-resulting in reduced costs and a solution that is better for the environment. When you consider that the average dental practice takes at least 384 impressions each year2, the positive impact is clear.


CS Connect

References
1 Edward J. Mills. A Clinical Method for the Diagnosis and Treatment Planning of Restorative Dental Patients, Journal of Oral Implantology. 2002;28(3):122-127.
2 Perry, Ronald. D. 2013. Time Is Money in Impressioning. Dental Economics. 103(8):56-57.










