Since the development of the high speed drill and ultrasonic instruments, dental professionals have been exposed to a biological aerosol that carries potential pathogens. Because of the aerosols generated by many instruments and procedures, dentistry as a profession poses a serious health risk for the professionals.
During the last 60 years, dentistry has addressed these concerns with personal protective equipment (PPE) and universal infection control measures. Current recommendations for PPE include an appropriate rated respirator or mask for the procedure, face shield, head cap, long sleeved gown, gloves, and shoe coverings to reduce the exposure and potential spread of infectious diseases (Figure 1).
Aerosols
Aerosols created by dental technologies and procedures have a long history in dentistry. They contribute to the health risk of dental professionals. In a report from 2017 examining 125,000 people in 974 different jobs and their risk for contracting a disease while at work, hygienists, dentists, assistants, and lab technicians occupied 4 of the top 5 spots.1 We tend to associate these risks with infectious diseases such as influenza or HIV/AIDS, and more recently SARS, or MERS. But this is only part of the story.
In 2015 the CDC released a report indicating dental professionals are 23 times more likely to contract and die from the rare and progressive lung disease Idiopathic Pulmonary Fibrosis.2 While not completely understood, it is believed that bacterial proteins inhaled from the aerosol contribute to this disease.
Dental aerosols were first studied and reported as early as 1969.3 The researchers defined aerosols as airborne droplets less than 50 microns in diameter. They examined CFU/min generated from numerous activities including, breathing, talking, coughing, sneezing and brushing teeth. Interestingly talking and breathing produced very few CFUs while sneezing and toothbrushing produce significantly more. But perhaps the definitive paper on dental aerosols was published in 2004.4
Harrel and Molinari described known diseases spread by droplets and aerosols, dental procedures that generate them, and best practices to reduce aerosol contamination. Obvious aerosol sources are the dental high speed drill and ultrasonic units, but also include air polishing, the air-water syringe, air abrasion, and hard tissue lasers.
The best strategies to reduce the aerosol risk include recommended PPE, HVE, preprocedural rinse, and high efficiency particulate air room filters. Extraoral HEPA vacuums can reduce the aerosol exposure to dental professionals (Figure 2). Multiple studies recognize the aerosol risks from the ultrasonic handpiece, and the importance of controlling the aerosol.5,6 There is conflicting data on whether routine use of rubber dams increases or decreases the aerosol risk.7
Pre-procedural Rinses
One significant way to reduce the potential health risk from the aerosol is to reduce the pathogenic burden in the aerosol. Pre-procedural antimicrobial rinses have been a standard practice in surgical implant procedures for many years, but the routine use of a pre-procedural rinse has only been given serious consideration since the COVID-19 pandemic.
Preprocedural rinses were first reported in 1976, examining the bacterial reduction potential of Chlorhexidine and Povidone Iodine.8 Both rinses significantly reduce bacterial load. Further studies compared the effectiveness of essential oils, chlorhexidine, and hypochlorous acid as pre-procedural rinses.9,10 In perhaps very prescient timing, a systematic review on pre-procedural rinses was published just prior to the outbreak of COVID-19.11 They examined 770 studies and included 13 studies on chlorhexidine, essential oils, and cetylpyridinium chloride. Overall, the use of a pre-procedural mouth rinse resulted in a mean reduction in the number of CFUs of 64.8% compared with control. None of the included studies presented a low risk of bias and some dental procedures result in dissemination of microorganisms in the aerosol in the dental office. The authors concluded that there is moderate evidence that pre-procedural mouth rinses significantly reduce the number of microorganisms in the dental aerosol.
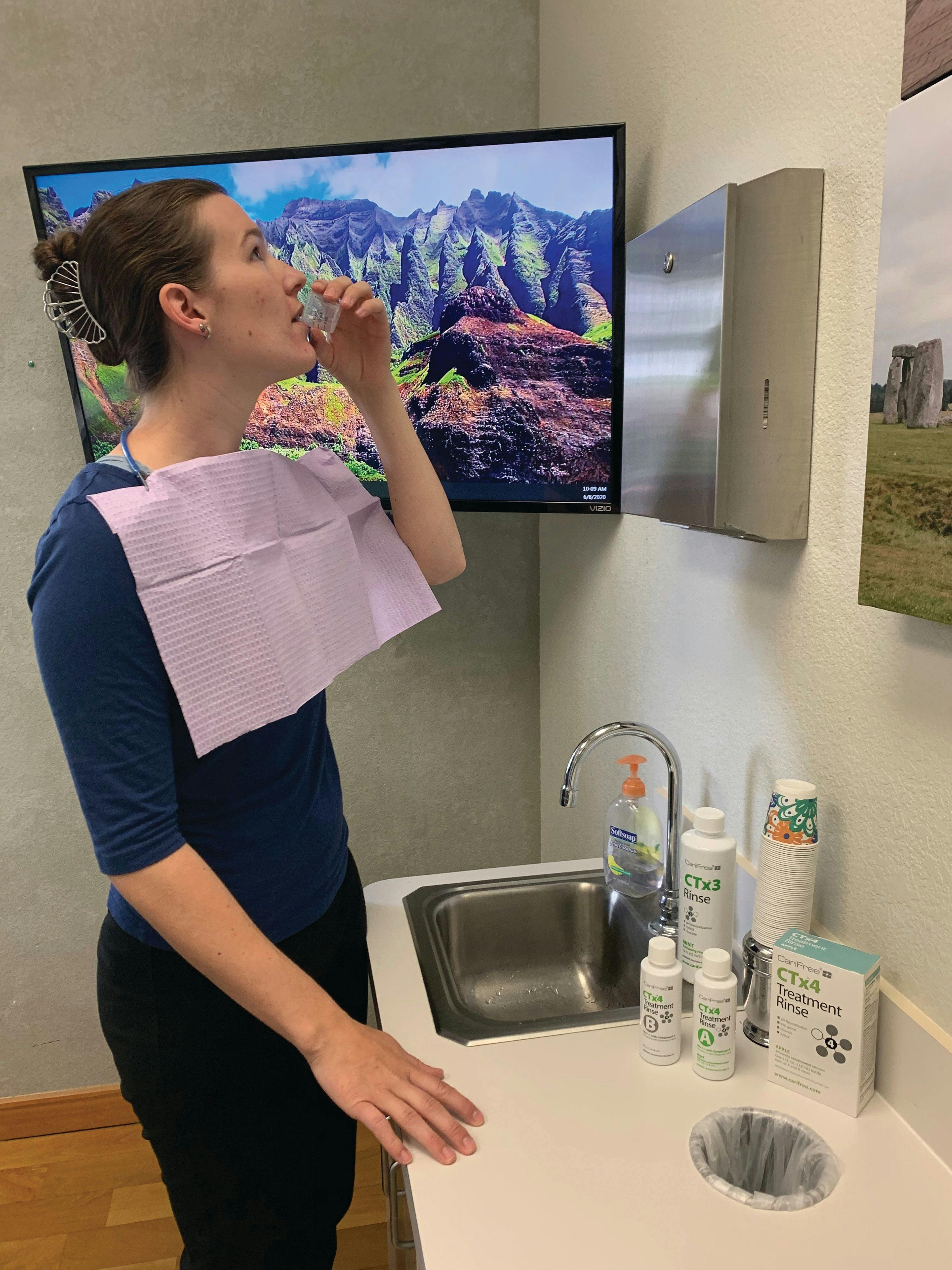
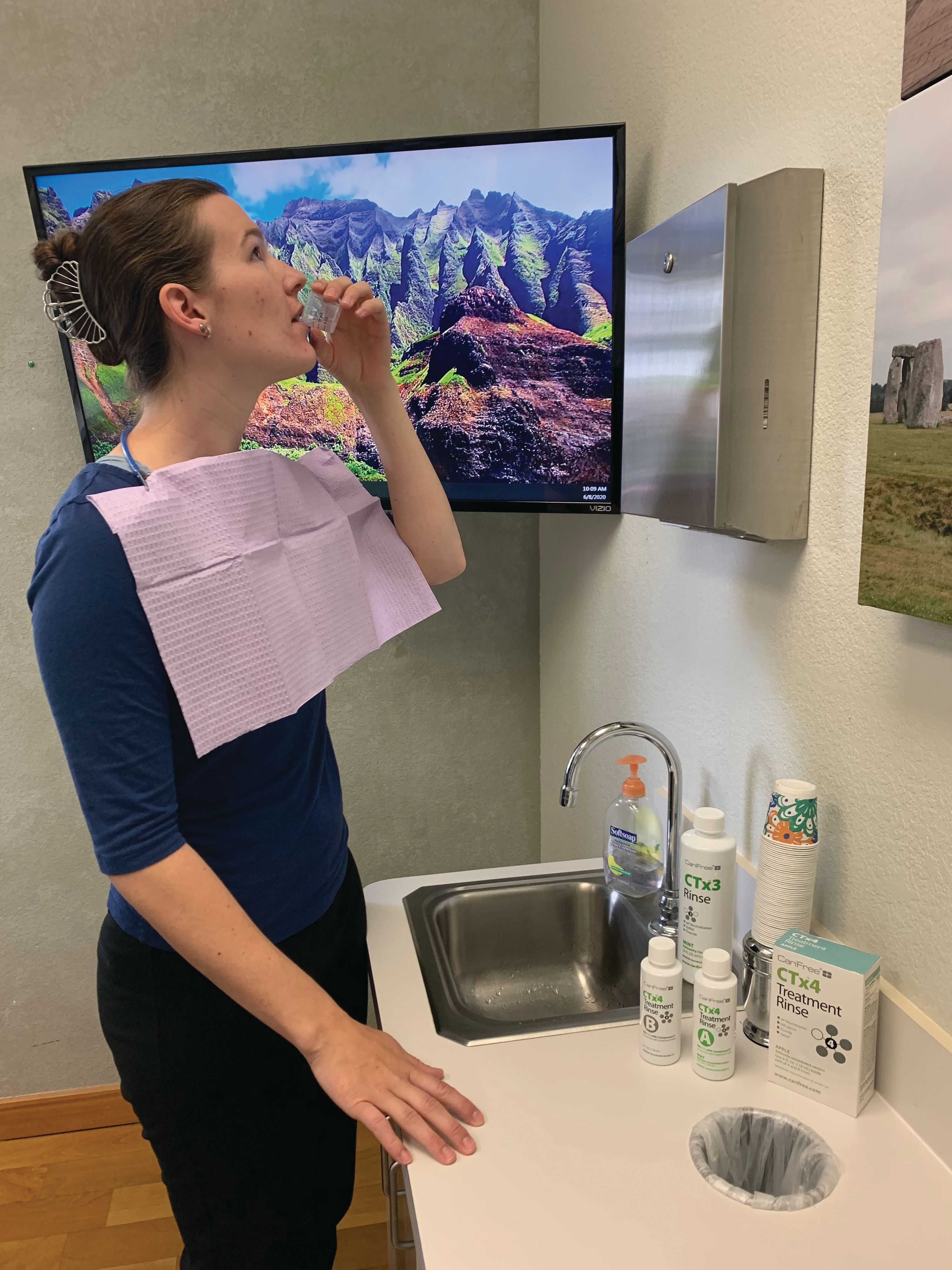
The use of a preprocedural rinse is an effective means to reduce the aerosol risk to dental professionals. It would also make logical sense for a patient to brush and floss their teeth prior to using the antimicrobial rinse to further reduce the microbial load in their mouth (Figure 3).
Sodium Hypochlorite Studies
Slots, et al, first reported on the use of sodium hypochlorite rinse as a self-care strategy in 2005.12 These antiseptics have significantly broader spectra of antimicrobial action, are less likely to induce development of resistant bacteria and adverse host reactions, and are considerably less expensive than commercially available antibiotics in controlled release devices.
CTx4 Treatment Rinse
- Designed to treat the cariogenic plaque biofilm.
- Reduces the overpopulation of cariogenic bacteria, and neutralizes oral pH.
- Intended for use by patients diagnosed to be at-risk for caries.
CariFree/Oral BioTech
866-928-4445 | carifree.com
Sodium hypochlorite is widely accepted as being a safe and effective antiseptic against bacteria, fungi, and viruses. For over a century, sodium hypochlorite has been used to control or overcome infection in homes, hospitals, and even on battlefields, and in endodontics for disinfection of root canals.13 In addition sodium hypochlorite rinse has been shown to be an effective antimicrobial rinse in the treatment of periodontal disease and dental caries, and increases remineralization.14,15,16 A commercially available rinse containing 0.20% sodium hypochlorite is the CariFree CTx 4 Treatment Rinse from Oral BioTech.
COVID-19 Studies
The COVID-19 pandemic created new challenges for the dental profession. COVID-19 is a very contagious disease transmitted by respiratory droplets. While no clinical trials have evaluated antimicrobial rinses and their direct effectiveness against this new coronavirus, available disinfection studies provide the best available evidence on effective antimicrobial agents against this virus.
When examining surface disinfection, the analysis of 22 studies reveals that human coronaviruses such as Severe Acute Respiratory Syndrome (SARS) coronavirus, Middle East Respiratory Syndrome (MERS) coronavirus or endemic human coronaviruses (HCoV) can persist on inanimate surfaces such as metal, glass or plastic for up to nine days, but can be efficiently inactivated by surface disinfection procedures with 62-71% ethanol, 0.5% hydrogen peroxide or 0.1% sodium hypochlorite within 1 minute.17 When examining coronaviruses and histopathology, experts are confident that 70% ethanol and 0.1% sodium hypochlorite should inactivate the virus.18
And finally, a handwashing study of the COVID-19 virus demonstrated that instant hand wiping using a wet towel soaked in water containing 1.00% soap powder, 0.05% active chlorine, or 0.25% active chlorine from sodium hypochlorite removed 98.36%, 96.62%, and 99.98% of the virus from hands, respectively.19 Based on this evidence, sodium hypochlorite is an effective antimicrobial agent against the COVID-19 virus.
Conclusion
Dental aerosols create serious health risks for dental professionals. The COVID-19 pandemic has been a long overdue wake-up call for the dental profession. We must up our game to reduce the health hazard risks for all dental professionals from these aerosols. The best means to do this is to reduce the potential infectious load of the aerosol with universal pre-procedural rinses and controlling the aerosol accessory high efficiency particulate vacuums.●
References
1. Business Insider 2017 Top 47 Unhealthy Jobs in America; https://www.businessinsider.com/most-unhealthy-jobs-in-america-2017-4
2. Nett RJ, Cummings KJ, Cannon B, Cox-Ganser J, Nathan SD. Dental Personnel Treated for Idiopathic Pulmonary Fibrosis at a Tertiary Care Center — Virginia, 2000–2015. CDC Weekly 2018. 67(9:;270–273.
3. Micik RE, Miller RL, Mazzarella MA, Ryge G. Studies on dental aerobiology. Bacterial aerosols generated during dental procedures. J Dent Res. 1969 Jan-Feb;48(1):49-56.
4. Harrel SK, Molinari J. Aerosols and splatter in dentistry: a brief review of the literature and infection control implications. J Am Dent Assoc. 2004 Apr;135(4):429-37.
5. Singh A, Shiva Manjunath RG, Singla D, Bhattacharya HS, Sarkar A, Chandra N. Aerosol, a health hazard. Indian J Dent Res. 2016 Mar-Apr;27(2):160-2. doi: 10.4103/0970-9290.183131.
6. Su J. [Aerosol transmission risk and comprehensive prevention and control strategy in dental treatments]. Zhonghua Kou Qiang Yi Xue Za Zhi. 2020 Apr 9;55(4):229-234.
7. Al-Amad SH, Awad MA, Edher FM, Shahramian K, Omran TA. The effect of rubber dam on atmospheric bacterial aerosols during restorative dentistry. J Infect Public Health. 2017 Mar - Apr;10(2):195-200.
8. Altonen M, Saxen L, Kosunen T, Ainamo J. Effect of two antimicrobial rinses and oral prophylaxis on preoperative degerming of saliva. Int J Oral Surg. 1976 Dec;5(6):276-84.
9. Logothetis DD, Martinez-Welles JM. Reducing bacterial aerosol contamination with a chlorhexidine gluconate pre-rinse. J Am Dent Assoc. 1995 Dec;126(12):1634-9.
10. Lafaurie GI, Zaror C, Díaz-Báez D, Castillo DM, De Ávila J, et al. Evaluation of substantivity of hypochlorous acid as an antiplaque agent: A randomized controlled trial. Int J Dent Hyg. 2018 Nov;16(4):527-534.
11. Marui VC, Souto MLS, Rovai ES, Romito GA, Chambrone L, Pannuti CM. Efficacy of preprocedural mouthrinses in the reduction of microorganisms in aerosol: A systematic review. J Am Dent Assoc. 2019 Dec;150(12):1015-1026.
12. Jorgensen MG, Aalam A, Slots J. Periodontal antimicrobials—finding the right solutions. Int Dent J February 2005. 55(1):3-12
13. Rich SK, Slots J. Sodium hypochlorite (dilute chlorine bleach) oral rinse in patient self-care. J West Soc Periodontol Periodontal Abstr. 2015;63(4):99-104.
14. Slots J. Periodontitis: facts, fallacies and the future. Periodontol 2000. 2017 Oct;75(1):7-2316.
15. Hallett KB, O'Rourke PK. Baseline Dental Plaque Activity, Mutans Streptococci Culture, and Future Caries Experience in Children Pediatr Dent . 2013;35(7):523-8.
16. Fernando JR, Shen P, Walker GD, Yuan Y, Stanton DP, et al. Effects of Bovine Serum Albumin and High pH Pre-Treatment on the Remineralization of Enamel Subsurface Lesions in vitro. Caries Res. 2020;54(1):36-42.
17. Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J Hosp Infect. 2020 Mar;104(3):246-251.
18. Henwood AF. Coronavirus disinfection in histopathology. J Histotechnol. 2020 Mar 1:1-3.
19. Ma QX, Shan H, Zhang HL, Li GM, Yang RM, Chen JM. Potential utilities of mask-wearing and instant hand hygiene for fighting SARS-CoV-2. J Med Virol. 2020 Mar 31.