Overcoming Endodontic Hurdles With Restorative Products
Navigating complex endodontic procedures can be time-consuming and difficult, but products from Centrix aim to help.


Overcoming Endodontic Hurdles with Restorative Products. Image credit: © Centrix

A recent complex endodontic case resulted in an effective resolution of its clinical challenges. This case study describes how 2 restorative products significantly aided precision, efficiency, and overall clinical outcomes. The difficulties encountered underscore how the mechanical and handling properties of the chosen dental materials were crucial to the successful outcome of the clinical tasks.
Case Presentation and Diagnosis
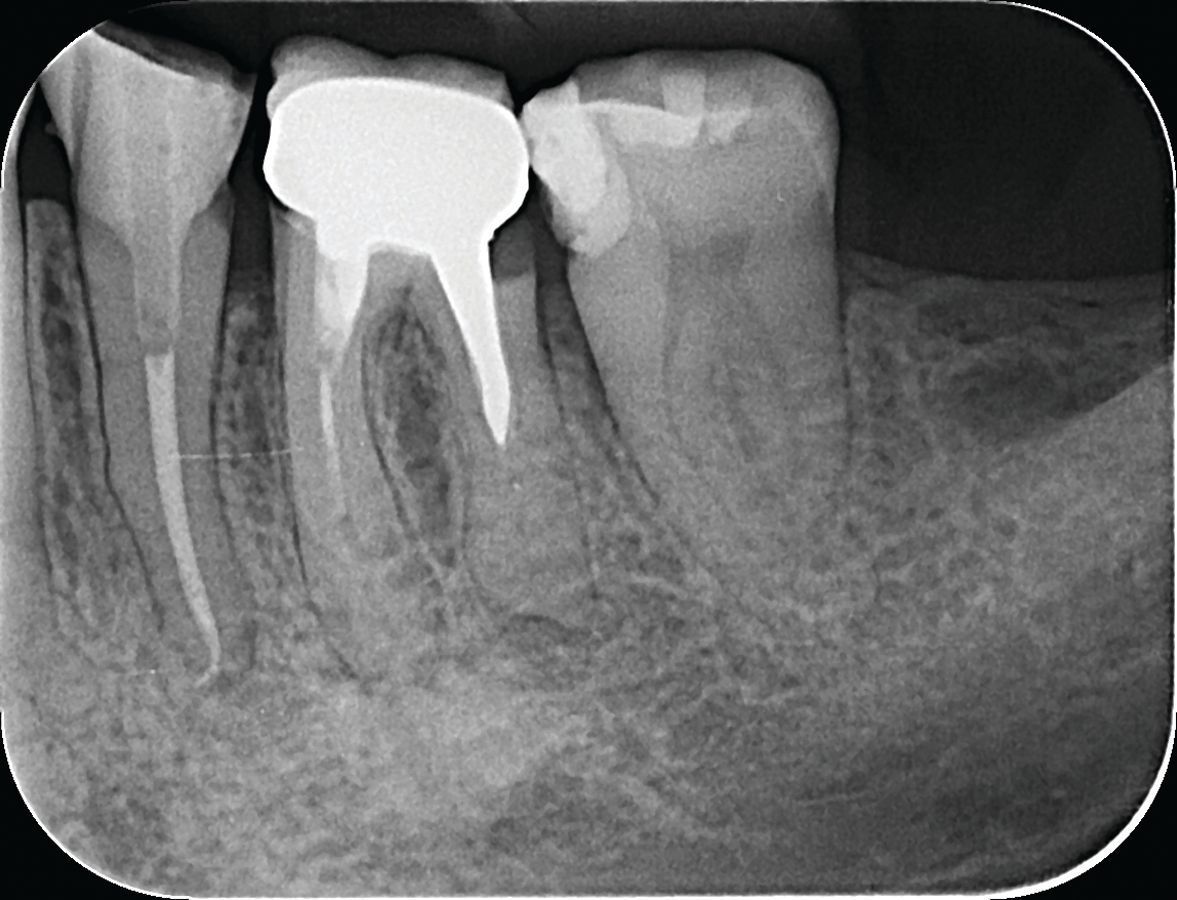
A 46-year-old woman presented to our dental clinic complaining of pain during chewing and a persistent “bad smell” emanating from tooth #19. Radiographic examination revealed a periapical lesion and subgingival distal decay (Figure 1). Additionally, the tooth was tender upon percussion, indicating an acute issue that needed immediate attention.


Figure 1. Radiograph of tooth #19 with pre-existing crown, visible periapical lesion, calcified canal and subgingival distal decay.
Upon further evaluation, the unique challenges of this case became apparent. Difficulties included as follows:
- Presence of a calcified root canal
- Substantial size of an existing metallic cast post necessitating its intricate removal, and
- Difficult access to the distal decay at the subgingival level.
Treatment recommendations included removing the preexisting crown, root canal therapy, and tooth reconstruction to prepare for the fabrication of a new crown.
Treatment Process
The treatment procedure involved 4 critical objectives: addressing subgingival caries, removing the cast post, building up the core, and starting root canal therapy. Our first step involved the atraumatic removal of the preexisting crown and exposing the cast metallic post, which had to be cut in half and removed. A gingivectomy was performed to access the distal subgingival decay using a ceramic bur without coolant to aid tissue hemostasis. A rubber dam was placed prior to the core build-up and reconstruction of the distal wall.
Initial Visit
Due to the significant coronal destruction, a contrast core build-up material was used to restore structure to the tooth. In our endodontic practice, core buildups are a natural extension of root canal treatment to ready the tooth for permanent restoration by the general dentist or prosthodontist. In the posterior region, a contrasting core buildup shade of blue can enhance visibility, underscoring the need for continued treatment (Figure 2).


Figure 2. Reconstruction of tooth with Encore D/C contrast shade core build-up.

It is a deliberate choice to use a contrasting blue-colored material as opposed to using a conventional white or tooth-colored shade; the blue-colored tooth creates a clear reminder to the patient that treatment is not yet complete and that the tooth still needs a permanent crown. In reality, some patients may only return to restore their “blue” tooth with a crown for purely esthetic reasons, in which case the mission of having the patient return to the restorative dentist for crown fabrication is complete.
Problem Solver
A contrast dual-cure, core buildup material (Encore D/C MiniMix from Centrix) was selected for several reasons. The working properties of this material allow it to hold shape without slumping and eliminate the need to use a matrix or core form. The same material can be used for the buildup of a coronal core and the fabrication of a composite post and core, bonding the post, tooth, and core together into an integrated whole. The material is available in small, unique, prefilled 0.5-mL compules with an extended mixing tip for easy access and application down canals in the second and third molars. This small format dispensing system was most helpful in the core buildup for this case.
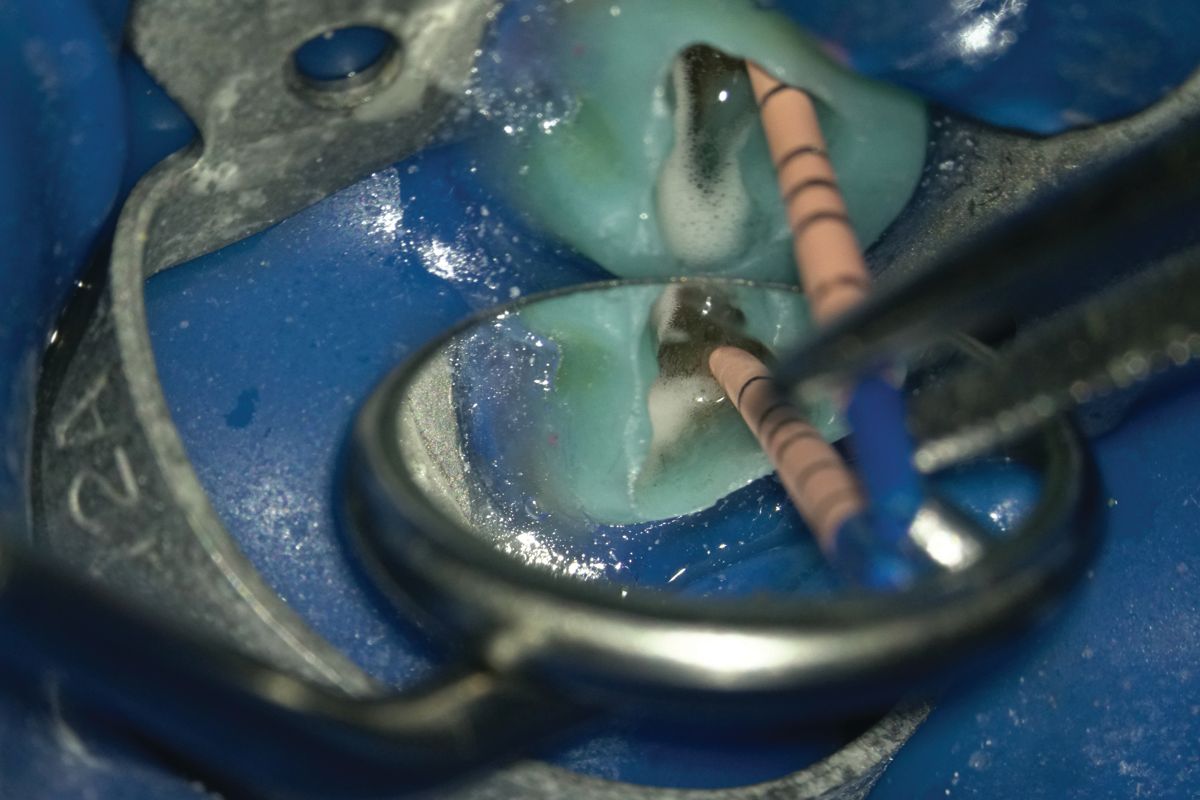
Upon completion of the contrast core buildup, root canal therapy was initiated (Figure 3).

Figure 3. Initiating root canal treatment after completing contrast core buildup.

Unfortunately, removing the metallic cast post took more time than expected, limiting our capacity to thoroughly address root canal disinfection and treatment at this appointment. As an interim measure, calcium hydroxide was placed in the canals.
Another Problem Solver
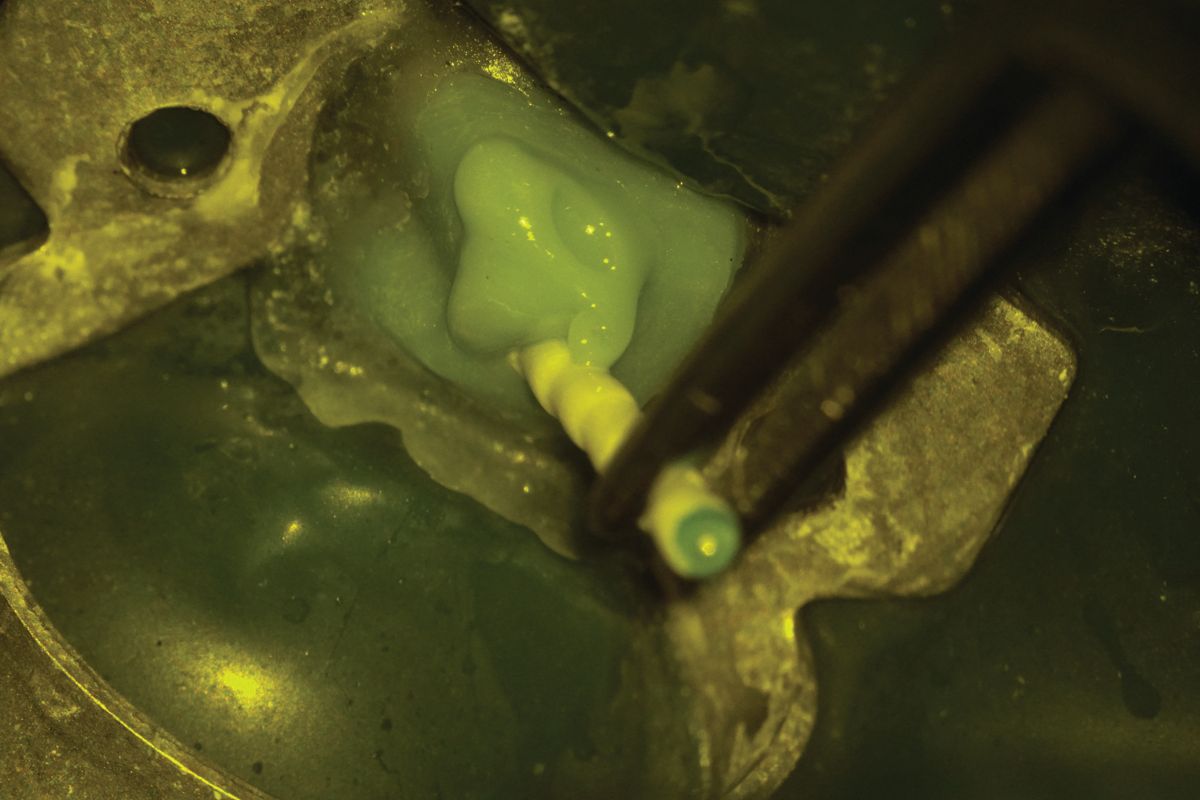
The access opening was then filled with a moisture-activated temporary filling and sealing material (Tempit® from Centrix) containing calcium sulfate and zinc oxide (Figures 4 and 5).

Figure 4. Tempit temporary material filling and sealing the access opening after placement of calcium hydroxide.


Figure 5. Rubber dam placed, Tempit removed. Continuing root canal treatment on tooth #19 with warm vertical obturation.
The material expands while absorbing moisture, causing slight expansion during curing and perfectly sealing the cavity. Tempit was chosen for its performance benefits and its endurance over time. The antibacterial properties of Tempit (ie, zinc oxide) were essential in this case because time did not allow for sufficient root canal disinfection.
Since the material dispenses from prefilled tips, there is no mixing or dispensing from jars, eliminating the risk of cross-contamination or premature setting. Additionally, the viscosity of the material is consistent each time, so it can be delivered precisely to the prep, flowing into the cavity from the bottom up, eliminating any voids. Tempit’s mechanical properties exhibit high strength with low wear, which was evident when the patient returned for the second visit.
The Return Visit
In between visits, the patient did not experience any episodes of pain. The Tempit filling was intact, exhibiting no staining from bacterial contamination. A critical mechanical property of this material is its endurance over time. Once set, it shows superior retention and holds up to masticatory forces. Although Tempit is very strong once set, its removal is easiest using an ultrasonic scaler rather than using an explorer. Moreover, the ultrasonic scaler is faster, more efficient, and significantly safer than using a bur to remove temporary fillings in endodontic situations as it avoids the risk of removing sound tissue.
The process of disinfecting and treating the root canals was completed. A self-etch, dual-cure bonding material was applied within the initial core buildup and the canals. After dispensing the Encore D/C dual-cure buildup material into the distal canal, a glass-fiber post was positioned (Figure 6).

Figure 6. The buildup after cleaning the sealer, partial obturation, and preparing for the glass fiber post placement in the distal canal.

Working through a microscope, the orange-colored light filter was activated on the microscope to prevent the white light of the microscope from prematurely curing the material, thus allowing adequate time to place the glass-fiber post (Figure 7).

Figure 7. Orange light prevents accidental curing.
Using a self-etch dual cure bonding material facilitated the bonding of Encore D/C to the tooth structure, the glass-fiber post, and the previously placed core buildup, making everything a monobloc. As curing continued, the initial contrast Encore D/C core buildup now became part of the final core buildup. Any excess material was removed with a bur when all materials were cured.
The final x-ray shows the completed root canal treatment, restored subgingival distal carious lesion, and glass-fiber post (Figure 8).


Figure 8. After completion of root canal treatment, repair of subgingival carious lesion, core buildup and glass fiber post in distal root of tooth #19, in preparation for permanent crown.

In this clinical situation, Encore D/C and Tempit proved to be problem-solving products that contributed to the successful outcome of this challenging case.

















