How to use Planmeca Extraoral Bitewings to detect cysts
Utilizing multiple patient assessment options can lead to expanded patient care.

Effective patient assessment is critical to the delivery of high-quality dental care. Patient assessment sometimes extends beyond the boundaries of the oral cavity, thus requiring additional “care” or “consideration” be taken.
Case study
One such situation involved a healthy 61-year-old patient who had a history of adamantly resisting routine dental X-rays. Her abnormal fear of ionizing radiation, in particular a fear of X-rays, is called radiophobia.
During previous routine check-ups, the patient had been advised of a possible cyst formation around the retained impacted 3rd molars and the need to monitor them through annual X-rays.
Related article: How to get the perfect X-ray for you
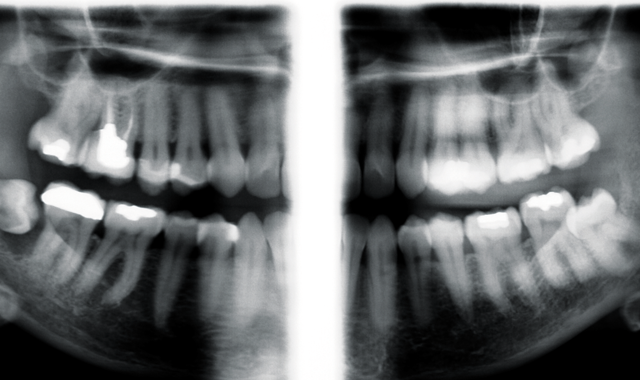
The patient was in the office in 2006 for a routine check-up and consented to a panoramic X-ray. The X-ray revealed no pathology associated with the #32 tooth. The patient was informed of the risk of cyst development associated with the impacted third molar, which would include the possibility of temporary or permanent damage to the inferior alveolar nerve.
During routine examinations over the next seven years, periodontal probing revealed no communication from the oral cavity to the impacted wisdom teeth.
Up next: How the patient was treated
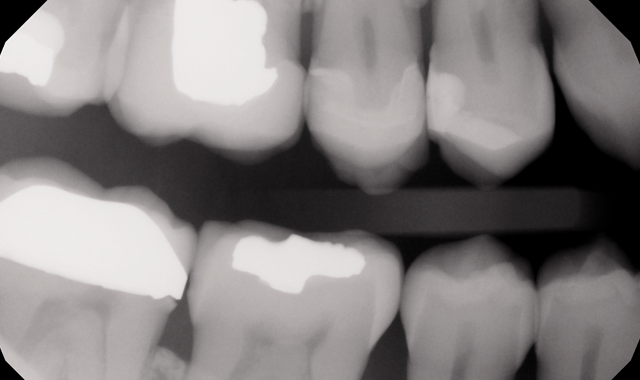
The patient agreed to intraoral digital bitewings in 2013. The scope of this X-ray is limited, as is their size and thickness. At the time these X-rays were taken they provided no diagnostic information about the wisdom teeth. Recalling this patient’s radiophobia, the possibility of doing retakes was not pleasant.

Routine panoramic X-ray


Image of digital intraoral bitewings
Further examination was deemed necessary, but instead of conducting more intraoral bitewing X-rays, extraoral bitewings were discussed with the patient. Again, taking into consideration the patient’s radiophobia, the adjustable mA and kV would allow the optimal radiation dose, while adhering to the ALARA (As Low As Reasonably Achievable) principle. The benefit to the patient would be that extraoral bitewing X-rays would provide the necessary imaging with a substantial reduction in radiation exposure versus taking four intraoral bitewing X-rays to cover the same area in question-thus helping to ease the patient’s concern regarding exposure to radiation.
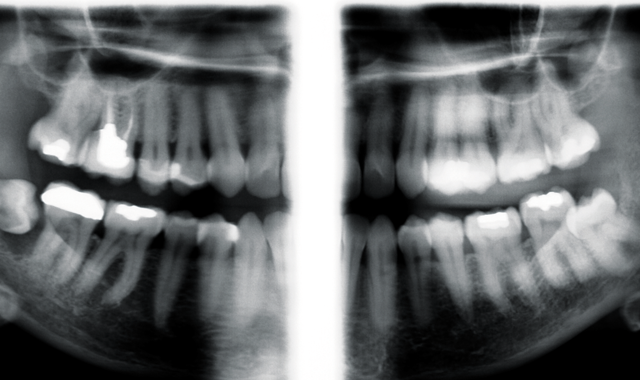
Planmeca extraoral bitewing follow up X-rays were taken in 2015, utilizing Planmeca’s exclusive robotic SCARA (Selectively Compliant Articulated Robot Arm) technology. As a result, additional periapical regions, including the 3rd molar areas, were now able to be included in the images.
Image of Planmeca extraoral bitewings

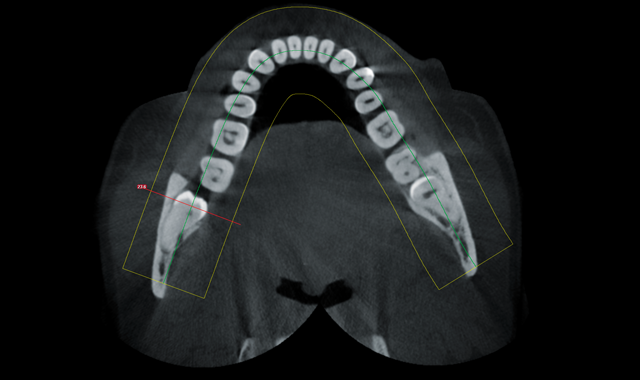
Axial view
From the expanded regions available via extraoral bitewings X-rays, the cyst around the #32 tooth was discovered. The patient was informed of the need to have the wisdom tooth removed, and the possibility of damage to the inferior alveolar nerve and permanent paresthesia.
After seeing the large lesion on the extraoral bitewing associated with #32 tooth the patient quickly consented to a 3D CBCT of both lower third molar areas.

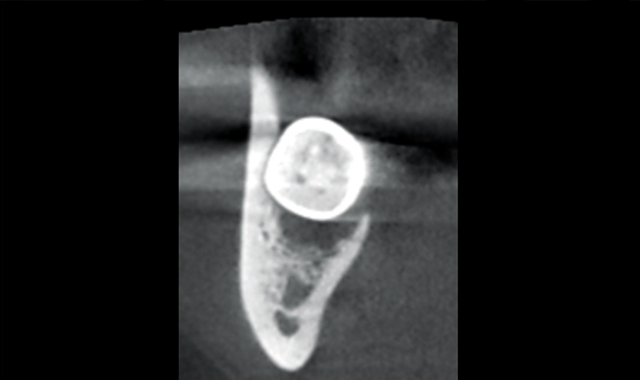
Coronal view showing proximity of nerve and coronal portion of tooth

Coronal view showing extent of lesion and proximity of nerve and apical portion of root
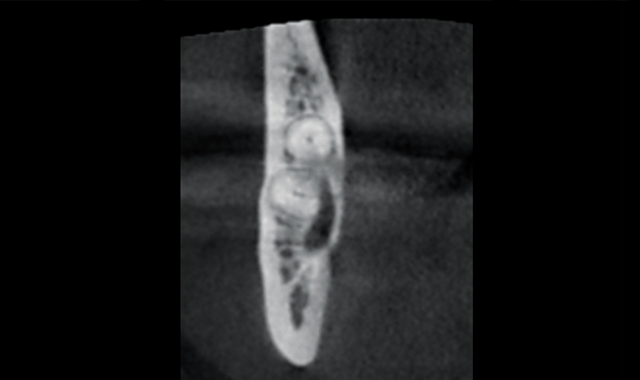
Through the use of 3D imaging, the patient had a much better understanding of the complexity of the issue. The coronal view of the #32 tooth shows the involvement of the lesion and the distance from the nerve to the coronal portion of the tooth. The improved distal slice shows the extremely close proximity (of lesion) to the mandibular nerve and the apical portion of the root.
The patient, along with the CBCT, was referred to an oral surgeon for consultation and removal of the #32 tooth. The tooth was removed without any complications.
Conclusion
Having access to 2D and 3D radiography in the general dental office provided increased diagnosis capability, treatment acceptance and ultimately a successful outcome for the patient.










