How low-carb diets impact oral health
One of the longest trends in appetite control has been the low-carbohydrate diet.



One of the longest trends in appetite control has been the low-carbohydrate diet.
Many patients, when filling out their medical, dental and personal history, reveal they follow these patterns of eating. Nutrition may have stabilizing or damaging effects on the oral cavity, so as registered dental hygienists, we are in the perfect position to discuss the effects of low-carb dieting on the oral cavity, including the topic people are most embarrassed about: halitosis.
Theoretically, when shrinking your waistline, there should be a reduction in the occurrence of carious lesions. Fermentable carbohydrates, especially sucrose, are absorbed by biofilm. This process causes bacterial plaque to produce acids.1
Frequent exposure of a susceptible tooth surface to the acid causes demineralization, the initiation of the caries process.2 Progressive, intermittent demineralization of the tooth structure may progress into complete destruction of coronal dental tissues and development of pulpal abscesses.

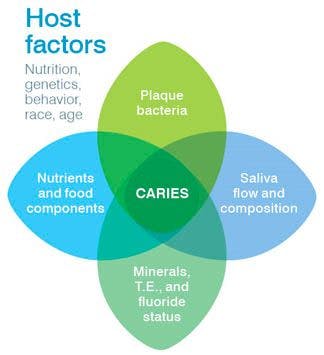
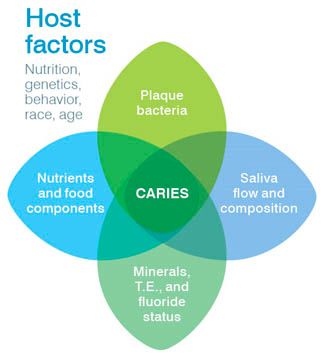
Where caries come from
The etiology of dental caries is multifactorial. The chart to the left offers a visual guide. Streptococcus mutans and lactobacilli are bacteria found in biofilm that are highly cariogenic. Their cariogenic action has four aspects considered as separate effects:3
Implantation mechanism involving adhesion.
Colonization through competition with other bacterial components.
Metabolic activity of established bacteria under the influence of food residues and oral environment.
Increased thickness of plaque and its control by oral hygiene.
How can we help
our patients?
Recommend to your patients the following suggestions by the Academy of General Dentistry:
- Drink plenty of water
- Chew sugarless gum with Xylitol or suck on sugarless mints
- Brush and floss after every meal
Advise your patients that these recommendations may help mask bad breath, but will only have a temporary effect on malodor until the source is remedied.
Saliva acts as an important protective fluid in the oral cavity. In conjunction with plaque, it contains minerals and trace elements such as fluoride, calcium and phosphorus that contribute to the remineralization of enamel. Calcium and phosphorus also are useful in the maintenance of the supportive alveolar bone.
The pros to low-carb…
Food residues, specifically carbohydrates, have caries promoting characteristics that allow fermentation and acid accumulation to occur in bacterial plaque.3 It enhances the four previously mentioned activities of biofilm: implantation, colonization, metabolic activity and thickness. When carbs are restricted in a diet, it limits an essential factor for the development of caries.
The Vipeholm study4 in 1954 first established the strong relationship between consumption and dental caries. It was supported by the investigation of Sreebny5 in 1982, which described the extensive reviews on the study, reaffirming its results. The literature concluded that a very low intake of sugar showed very low caries scores, and those that included a very high amount of sugar in their diets developed high numbers of carious lesions.
Dietary sucrose also may have an effect on plaque accumulation and bacterial population. The results of a study conducted by Carlsson and Egelberg6 found plaque formation during intake of sucrose was much thicker and heavier than that formed during glucose supplementation. Various studies7,8,9 have concluded a reduction in the amount of lactobacilli and/or streptococcus mutans in plaque and saliva when sucrose intake is low, and an increase in these microorganisms during a sucrose-rich diet.
…And the cons
Restricted carbohydrate intake also may have a negative effect on the oral cavity. It encourages the breakdown of fat stored for energy instead of glucose, a process known as ketosis or dietary ketosis. The breakdown of fats results in three different molecules called ketones, two of which (acetoacetate and ß-hydroxybutyrate) can be used for energy by most body tissues. The third ketone, acetone, cannot be used by the body and is excreted in the urine and exhaled by the lungs, causing halitosis.10,11
Smelling the patient’s breath is the easiest and most commonly used method of detection. Normal breath of a healthy patient should have no odor or a slightly sweet smell. When the odor is not limited to the mouth, but also is recognized through the nose, it can be assumed that the odor may have a systemic or non-oral origin. Chronic oral malodor is a common dental problem and may cause patients to seclude themselves from social activities fearing the shame the condition brings.2
Remember to be sensitive to your patients’ concerns. If chronic halitosis persists and the patient is no longer on a low-carb diet, refer the patient to be medically evaluated because it can and should be a health concern. The modern hygienist is in a unique role to promote oral as well as systemic health.
Lisa Stefanou, RDH, BS, MPH, is assistant director of dental hygiene programs and associate professor at NYU College of Dentistry, New York.
Dianne Sefo, RDH, BA, is a full-time instructor in dental hygiene at the NYU College of Dentistry.










