How to choose the most suitable temporization approach
Temporization, or, as it’s often called, “provisionalization,” might be considered its own subdivision of restorative dentistry. Before we plan any type of dental rehab, we need to “pre-think” how we’ll maintain our patient’s appearance and function and keep him or her comfortable for the duration. We also need to decide on the particular technique, materials and cement we will use.
Temporization, or, as it’s often called, “provisionalization,” might be considered its own subdivision of restorative dentistry. Before we plan any type of dental rehab, we need to “pre-think” how we’ll maintain our patient’s appearance and function and keep him or her comfortable for the duration. We also need to decide on the particular technique, materials and cement we will use.
“Pre-think” is the operative term. We must know the specific requirements of our temporization in advance. Will it be worn for three weeks or three months? Will it need to be removed and recemented several times? Is the patient a bruxer? Are exquisite esthetics critical? What costs will the provisional add to the treatment plan? Must you involve a laboratory to generate a satisfactory result, or can a satisfactory result be had chairside?

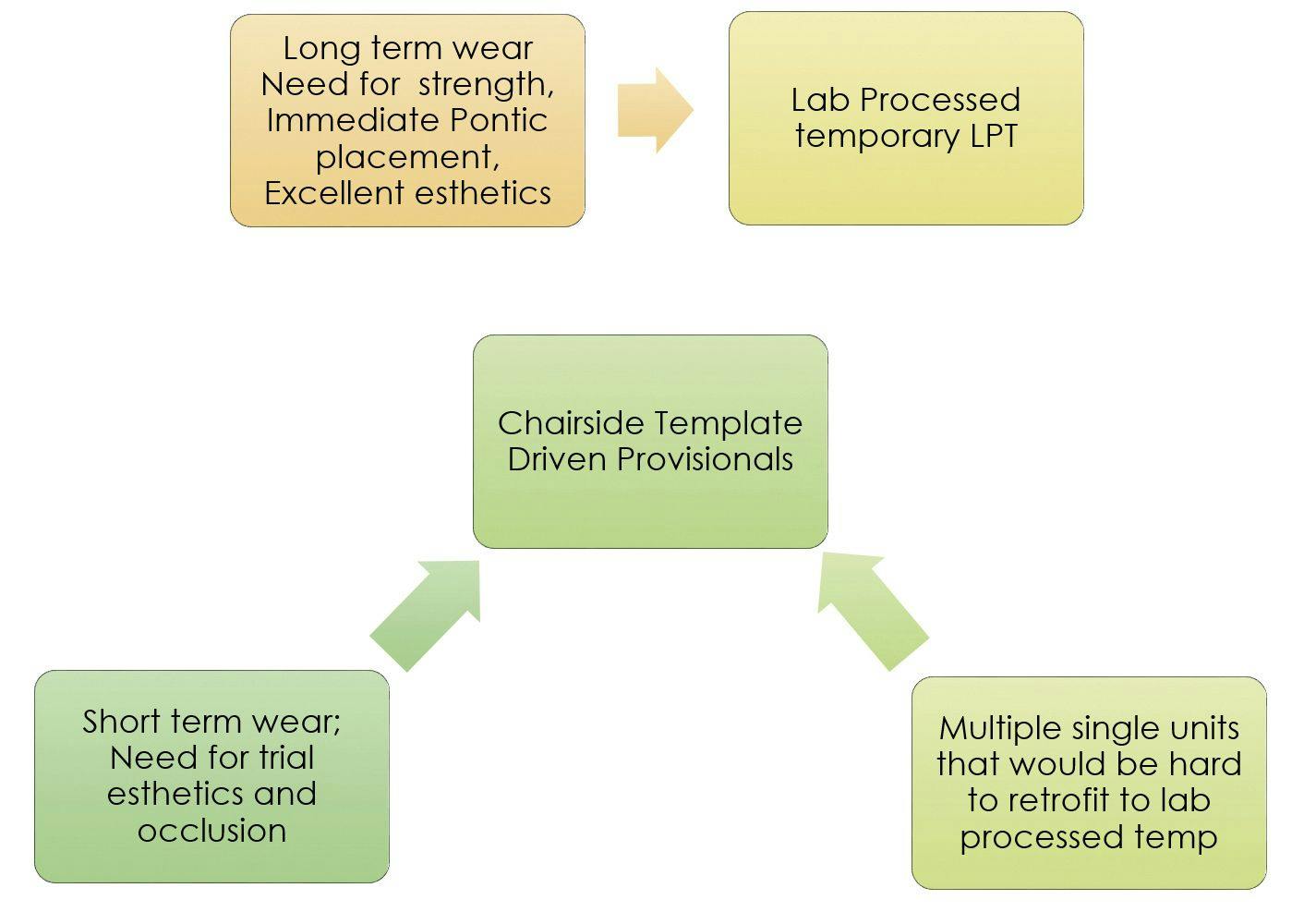
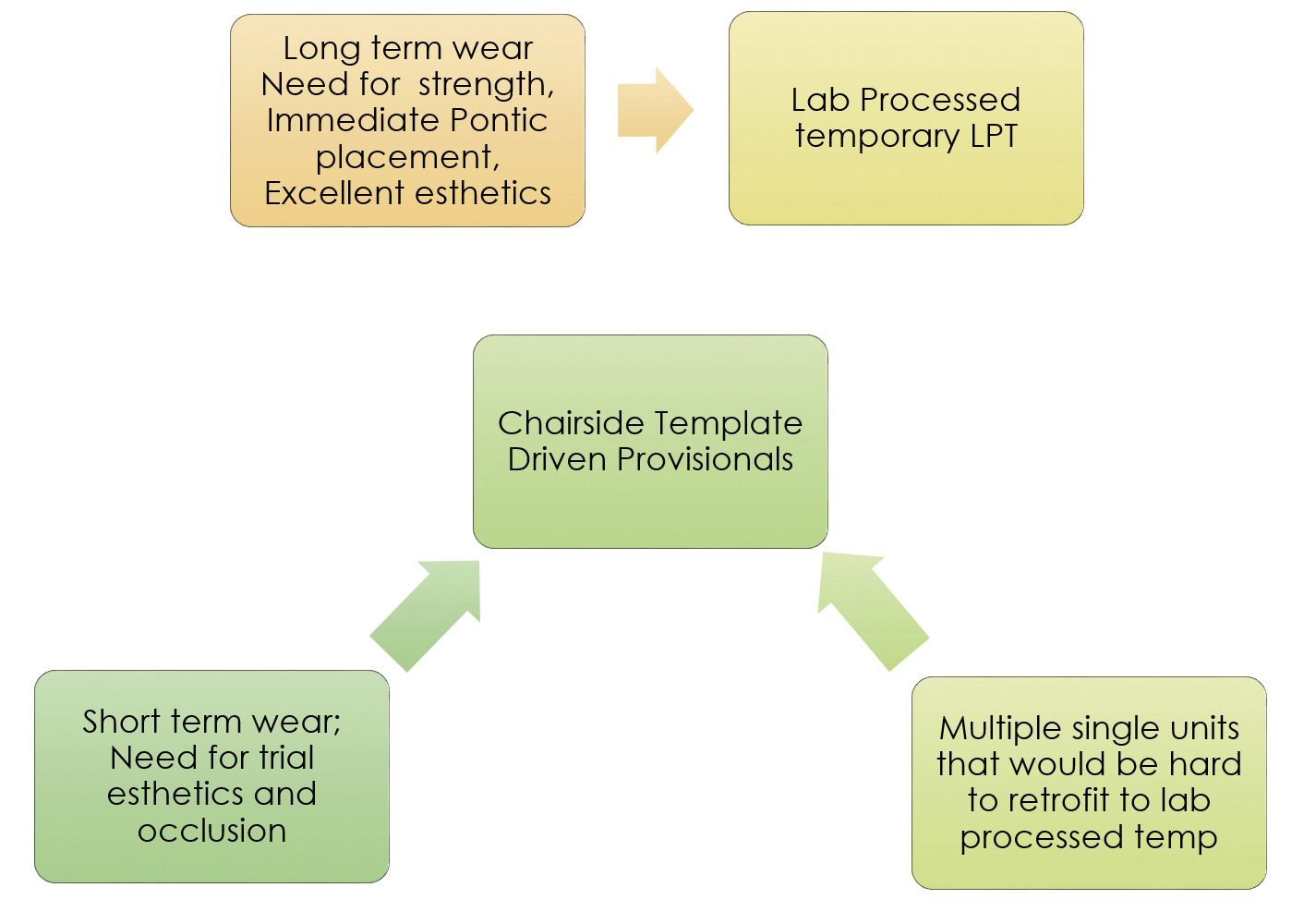
This figure outlines a simplified rationale for choosing the appropriate temporization technique for our smile rehab projects. It differentiates when a clinician might choose a laboratory-processed temporary and when a chairside-fabricated temporary might be more appropriate. The lower portion of the diagram focuses on the chairside, template-driven provisional, which is the focus of this article. Such indexed or template-driven provisionals, most likely fabricated from one of the many bisacryl formulations available today, are practical for short-term provisionalizations (three to six weeks).
Bisacryl materials, while excellent in appearance and handling, prove to be somewhat brittle and prone to leakage. This contributes to the lack of flexibility ascribed to this material class. Provisionalizations that feature several months of wear and multiple removal and recement cycles are often best served by lab-processed acrylic and its inherent toughness and flexibility. On the plus side, bisacryls may be easily added to or subtracted from when trial esthetics and/or occlusal schemes are planned. They are also easily repaired and marginated simply by applying appropriate amounts of your favorite composite.
And, finally, when multiple preps (i.e. four to eight) are to be included in your provisional, a template-driven technique using a bisacryl material is less difficult than attempting to match your own preps to your lab’s when employing a lab-fabricated provisional.
Watch the following video for a step-by-step case presentation:
Case presentation
In that vein, let’s examine a rather mundane (but frequently called for) chairside fabrication of a posterior three-unit temporary bridge. In this case, a span from Nos. 12 to 14 is seen pre-operatively, No. 14 having been compromised by recurring caries, as well as an intracoronal fracture. As the pre-operative anatomic form is suitable for “indexing” (i.e. creating a silicone matrix or template), and the temporary’s time in service will be limited to how long it takes to have the new bridge returned from the lab, a chairside bisacryl provisional would appear to be the perfect solution.


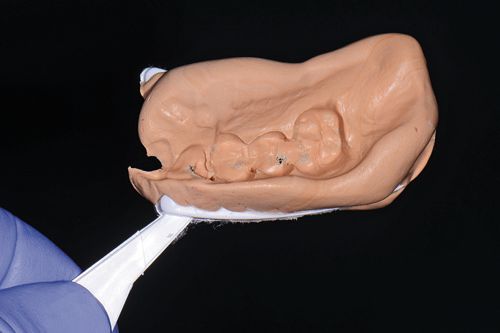
1. A silicone-based putty index was created by having the patient occlude into a triple tray filled with a silicone impression putty (Coltene’s Affinis® Putty Soft).
2. The built-up (No. 12) and prepared bridge abutments are prepared for provisional fabrication.
3. The VOCO Structur®3 bisacryl formulation is placed into the putty index with subsequent placement into the patient’s mouth. Structur®3 is a nano-filled bisacryl material said by the manufacturer to possess high fracture resistance and compressive strength (>500 MPa). It sets in 45 seconds intraorally. The manufacturer’s coined phrase “wipe and go” refers to the sheen obtained with the use of an alcohol wipe after one’s provisional has been trimmed. A natural gloss emerges as surface monomers are wiped away. Structur® 3 is available in eight VITA shades.
4. The newly minted, but still curing, provisional is gently trimmed with a No. 15 scalpel blade assisted by the firm putty backing.
5. The provisional is refined with an eight-bladed carbide finishing bur (Brasseler ET Finishing Bur #ET9). This proves to be the gentlest way to create accurate margins, particularly in thin zones of resin. Use of a heavier lab-style acrylic bur is more likely to overtrim or, even worse, fling your temporary into your trimmings pan.
6. The blade and finishing bur approach described here along with Structur®3’s “auto-polish” feature will eliminate the need to plant yourself at the lab bench to finish your temporary.
7. Regarding Structur®3’s relative shade accuracy, the VITA shade tab (right side of tab display) bears a strong resemblance to the shade of our new provisional. The shade, opacity and opalescence can vary between products of the same shade designation so operators should do their best to match the bisacryl brand to the task.


This figure demonstrates our finished provisional following cementation with VOCO’s Bifix® Temp, a new composite-based provisional cement featuring a translucent tooth shade that does not shine through the provisional restoration. The auto-mix cement self-cures in four minutes but allows for light-curing to accelerate the process. A particular note is the ability to employ the “tack-cure” technique, which makes cleanup of excess cement a breeze. Yet, another time-saving process.
Conclusion
A “pre-awareness” of the service needs of our provisionals, as well as handling and appearance characteristics of the materials we employ, allows us to streamline and improve our temporizations. Doing so reduces the number of patient distress calls reporting ill-fated temporary restorations that require immediate attention. Patient, doctor and staff will certainly benefit from being spared such inconveniences.
About the author
Dr. Goldstein, a fellow of the International Academy of Dento-Facial Esthetics and the Academy of General Dentistry, practices general dentistry in Wolcott, Conn. Recognized as one of the Leaders in CE by Dentistry Today since 2002, and for his expertise in the field of dental digital photography, he lectures and writes extensively about cosmetics and the integration of digital photography into the practice. He has authored numerous articles for dental periodicals in the United States and abroad. He can be contacted at martyg924@cox.net.










