The top 10 things you need to know about ICD-10
The new ICD-10 diagnostic code set will be implemented on October 1. So, what do you need to know? Here are the top 10 things that will make the transition to ICD-10 a little bit easier.



The change may seem intimidating, but it’s coming all the same: The new ICD-10 diagnostic code set will be implemented on October 1, 2015. The International Classification of Diseases, Clinical Modification Volume 10 (i.e. ICD-10) is required on all medical insurance claim forms. So, what do you need to know? Here are the top 10 things that will make the transition to ICD-10 a little bit easier.
1. Background on ICD-10
The World Health Organization adopted this volume of diagnosis codes in 1993. ICD-10 is a much more specific code set than ICD-9, and as you become more familiar with it you will notice it feels more like a health care data statistics code set rather than a billing code set.
2. What's changed?
Just like in ICD-9, the diagnosis codes reported on a claim form tell the story of why you did what you did (support medical necessity). With room for 12 diagnosis codes on the new claim form, carriers are expecting you to give a complete story and how you list diagnosis codes is integral to getting the claim paid. When filling out a claim form, the code listed in box 21 line A should be the diagnosis codes that best supports the reason “why” you performed a service.
Remember the number one rule of diagnosis coding: We are telling the story to the carrier as to why you performed the service that you did. We are not making up a story to get a claim paid. The information listed on the claim form must be supported by the documentation in the patient’s medical record.
Continue to page two for more...
3. Codes
In ICD-10, codes are much more specific. For example, here is a comparison of the codes from ICD-9 to ICD-10 as it related to dental caries:

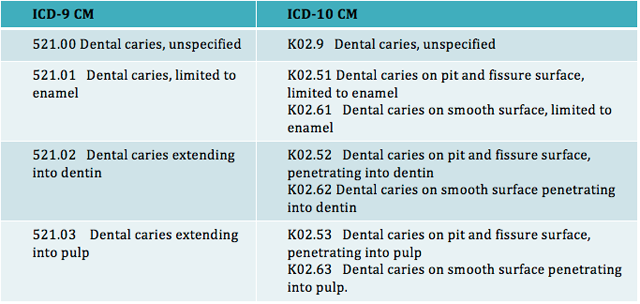
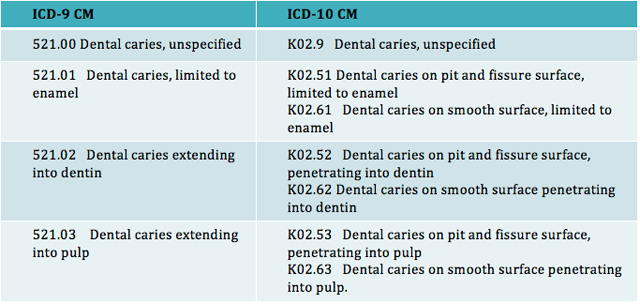
Due to the extent of the specificity of the codes, if you were to submit dental caries, unspecified, you are essentially reporting to the carrier that you do not have enough documentation in the patient record to correctly code the type of caries the patient has. This is definitely something you want to avoid, even with this transition rule or grace period. The code reported on the claim should be as specific as possible based on the documentation in the patient’s dental record and it should be complete based on the code set
4. Transition period
Medicare is allowing a one-year “transition” period, basically stating that if you are within the correct category of codes, your claims will not be denied for non-specific codes. Previous to this transition rule we were told that due to the specificity of the codes in ICD-10 submission of an unspecified code could quite possibly be denied.
Keep in mind, codes that are incomplete (i.e. not going out to the full number of characters or the full code) will be denied even if you are in the right category. The AMA did make a joint statement with Medicare (CMS) when this transition rule was released, however, each individual commercial carrier can elect whether or not to allow this transition rule. I recommend either checking with your carrier or even better code as specific as possible based on the documentation in the patient record.
Continue to page three for more...
5. The seventh character
ICD-10 has a brand new concept of a seventh character. This character, when required, has to be reported in the seventh space of the code. However, there are many codes that do not code out to six characters, so a placeholder or dummy code of “X” was developed to hold the space. For example, the code for a fractured tooth is “S02.5 Fracture of tooth (traumatic).” If you look up the code and read the notes, it will tell you to be sure to code this out to seven characters. S02.5XXA is the diagnosis code to report “Fracture of tooth (traumatic),” initial encounter (A). The A is in the seventh space and the X’s are used to hold the space between the S02.5 and the letter A for the seventh character.
The seventh character is required for all traumatic diagnosis codes and the definition and choices of the seventh characters varies within sections of the codebook. You will have to review the code set to determine the correct code for you to report based on the patient’s diagnosis and phase of treatment. The seventh character is not required in all sections of the ICD-10 codebook; however, it is always required for any trauma related diagnosis coding (fracture of tooth, bone, lacerations, puncture wounds, etc.).
6. Running dual systems
You will need to run dual systems (ICD-9 and ICD-10), for a period of time, since the diagnosis code reported is based on date of service, not on the date the claim is submitted. Claims for dates of service prior to October 1 will be submitted using ICD-9 codes. For dates of service October 1 and thereafter, the claims should be submitted with ICD-10 codes. This means that if it is late December and you are still working on a claim for a date of service prior to October 1, you would appeal, resubmit, etc. using ICD-9 codes rather than ICD-10. Remember, this is always based on the date of service. One other note regarding dual systems: Only HIPAA-covered entities are required to implement ICD-10; workers comp and auto insurance carriers are not HIPAA-covered entities and they have the choice as to whether or not to require ICD-10 codes.
Continue to page four for more...
7. Telling the story in codes
External causes are not a requirement for all carriers; however, correct use of the codes will allow you to “tell the story” and get paid faster, without providing a narrative. The trauma-related codes are listed in chapter 19 of the book. Chapter 20 has a listing of the external causes codes (how did the injury occur, what was the patient’s activity at the time of the injury, where did the injury occur and what was the patient’s status at the time of the injury). By using correct coding I can tell an entire story to an insurance carrier without having to send in a narrative. Check out this scenario:
A 12-year-old boy fell at home in his yard while riding his bike. When he fell, he landed on a tree root and cut his lower lip. The patient now presents for evaluation. What are the ICD-10 codes?
- S01.541A Puncture wound with foreign body of lip, initial encounter
- V18.0xxA Pedal cycle driver injured in non-collision transport accident in non-traffic accident.
- Y92.017 Garden or yard in single family (private) house as place of occurrence for external cause
- Y93.55 Activity, bike riding
- Y99.8 Other external cause status (includes leisure activity)
I am able to tell the carrier why the patient was treated, how the injury occurred, where the injury occurred, what the patient was doing at the time the injury occurred and why they were doing it (i.e. civilian, military or work related). As a coding geek, I think that is pretty cool and the effort that is put in up front before the claim is submitted is going to prevent lots of headaches and paperwork later on.
8. Laterality
Another new concept in ICD-10 is the concept of laterality. For parts of the body that we have two of, there is a separate code for the right side, left side, bilateral or unspecified. For example, to report a laceration of the right cheek, initial encounter, the code would be S01.411A. To report a laceration on the left check it would be S01.412A.
Continue to page five for more...
9. Equivalency mapping
CMS has developed a general equivalency mapping that will map for you from ICD-9 to ICD-10. There are approximately 14,000 codes in ICD-9 and about 69,000 codes in ICD-10 so there are many codes that have a one-to-one mapping (there was one ICD-9 code and there is one ICD-10 code, for such as supernumerary tooth). There are others where there was only one ICD-9 code, but a possibility of up to 10 ICD-10 codes. For example, loss of tooth due to trauma, ICD-9 code 525.11 becomes one of the following in ICD-10:
- K08.111 Complete loss of teeth due to trauma class I
- K08.112 Complete loss of teeth due to trauma class II
- K08.113 Complete loss of teeth due to trauma class III
- K08.114 Complete loss of teeth due to trauma class IV
- K08.119 Complete loss of teeth due to trauma unspecified
- K08.411 Partial loss of teeth due to trauma Class I
- K08.412 Partial loss of teeth due to trauma Class II
- K08.413 Partial loss of teeth due to trauma Class III
- K08.414 Partial loss of teeth due to trauma Class IV
- K08.419 Partial loss of teeth due to trauma, unspecified
10. Learning ICD-10 codes
The mappings are quite helpful but they are not a total substitute for learning ICD-10 codes. There are some concepts in ICD-10 that do not exist in ICD-9. Unspecified codes will link to unspecified codes, when in fact there is quite possibly a very specific code in ICD-10. I like to think of the mappings as similar to my car navigation system. Sometimes it brings me right to the front door of where I need to be; other times it just gets me in the general vicinity and I have to do some more investigation on my own to find my location.
Continue to page six for more...
Conclusion
As daunting as this may sound, I can assure you the more I work with this code set and the more I teach it, the easier it becomes. There is much less guessing with the new code set and there is literally a code for everything. I encourage you to embrace it as much as possible rather than fighting it.
The most important thing to remember about ICD-10: my mantra: “Keep Calm and Code On”
About the author
Terri’s extensive hands-on experience (over 30 years), including management of a multi-doctor Oral and Maxillofacial Surgery practice, laid the foundation for her current success as a practice management speaker and consultant and medical coding expert. She is certified by the American Institute of Healthcare Compliance, Inc as an ICD-10 CM Certified Trainer. For more information please visit the website www.terribradleyconsulting.com










