Technique: How technology opens up new opportunities for dental labs
Jason Atwood of Core3dcentres explores how the digital workflow opens up new avenues of income and expertise for dental technicians.
The explosive growth of digital technology in all facets of the dental industry has made even closer communication and cooperation between clinician, technician and in some instances, specialist the new reality. At the same time, whole new realms of materials, techniques and technologies have opened up within what the dental laboratory can now provide to the practitioner.
Trying to stay ahead of the trends and advancements is a daunting task for any individual. By including a lab that has integrated a digital workflow as just one part of the total solution, a dentist doesn’t have to worry about being left behind by new innovation.
Digital Esthetics discovers what digital advances REALLY mean for dentistry


Traditionally, the dentist would discuss and plan restorative options with the patient alone. Decisions were made on esthetic options, type of material, costs and even schedules. These decisions were all made chairside without input from the dental lab or a technician. Then, with these decisions in place, the dental technician and the lab team would make things work with quality restorations. While, more often than not, the final result was a success, today’s new technologies have made it possible for this time-honored system to be vastly improved with much better communication and technician involvement in an advisory capacity at the outset, to the positive benefit of clinician and patient alike.
Dentists can now take advantage of the knowledge and training of an experienced dental lab technician to plan and execute a complete restorative solution. Let’s look at just a couple of examples of technologies (virtual wax ups and digital surgical guides) where the technician can be involved in the planning stage of the restorative workflow.





Fig. 1 Traditional Diagnostic wax up.

Fig. 1 Traditional Diagnostic wax up.
Traditional Diagnostic wax ups (Fig. 1) were provided to help the patient make a more informed decision on the planned restorative work. While these certainly help the patient to envision what their new teeth may look like on a model, they cannot show the patient what they will look like in their own mouth.




Fig. 2 Digital wax up.

Fig. 2 Digital wax up.
Digital technology can take that imaging one step further and show the patient what those new teeth may look like by superimposing virtual restorations onto a photo of themselves. (Fig. 2) This technique is being called “emotional dentistry” but I suggest it is more than that. This new technology and technique really allows the patient to make a more informed and knowledgeable decision than was previously possible with traditional methods. For many patients who undergo complex restorative work, the journey can be a stressful one when you are unsure of the final destination. Those stresses are lessened when you have a clearer picture of your destination before you set out, making it easier for clinician and patient alike. Think about when you use a travel tool like Google Maps. When you reach your destination, and the outcome is indeed what you had envisioned, your reaction may well be a positive and emotional one.
Q&A: Jason Atwood on advances in implantology
Digital guided surgery is another area where the lab technician can be resource for the dentist. Using sophisticated software, a trained technician can merge a CBCT scan of the patient with either an intraoral digital scan of the mouth or a digital lab scan taken from a traditional impression. This merging creates a three-dimensional virtual model of the patient's skull, including the interior of the mouth. The technician can then, with input from the doctor, plan the placement of the implants into the virtual model. As this planning is done in a virtual environment, there is no need for the doctor to learn how to use, or to purchase, the required software. All the doctor needs is access to a computer to be fully involved in the process. They can choose to log in to a live online planning session with the software- trained technician, or they can use emaill to communicate with one another.
The “digital team” can discuss the final restorative goals as well as the surgical requirements and plan accordingly. Once decisions are made, and implants have been placed digitally as agreed, the surgical guide (or stent) can be designed from the digital model that now includes the depth, size and angles of the planned implants. A surgical guide is then fabricated in an acrylic type material, typically in one of two ways: by using a Computer Numerically Controlled (CNC) milling machine or by using an additive manufacturing process commonly known as 3D printing.

Fig. 3 Radiographic template denture.

Fig. 3 Radiographic template denture.
A Case History
A recent case that was planned with Dr. Vic Kooner of Bayview Dental in Qualicum Beach, British Columbia, Canada, was a great success using 3Shape Implant Studio. The patient was fully edentulous and had been using traditional dentures for over 20 years. Duplicates of his existing dentures were made and fitted. Radio opaque markers were imbedded into these duplicate dentures (Fig. 3) and two CBCT scans were conducted.

Fig. 4 Actual scan with dentures in place in patient's mouth. Note how the radio opaque markers are the only thing visible of the denture.
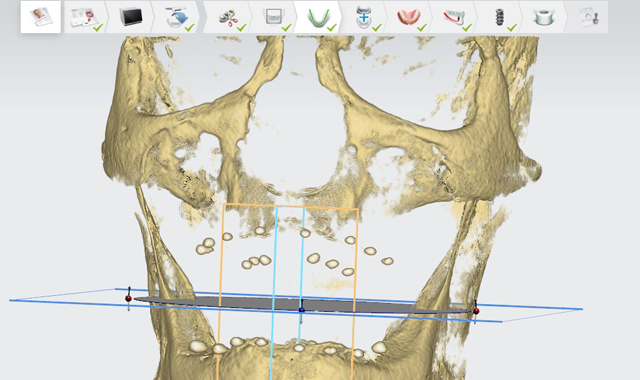
Fig. 4 Actual scan with dentures in place in patient's mouth. Note how the radio opaque markers are the only thing visible of the denture.
The first scan was done with the dentures in place in the patient’s mouth while biting down with moderate pressure to ensure they are in a ‘locked’ position. (Fig. 4)

Fig. 5 Second scan of individual denture appliances.
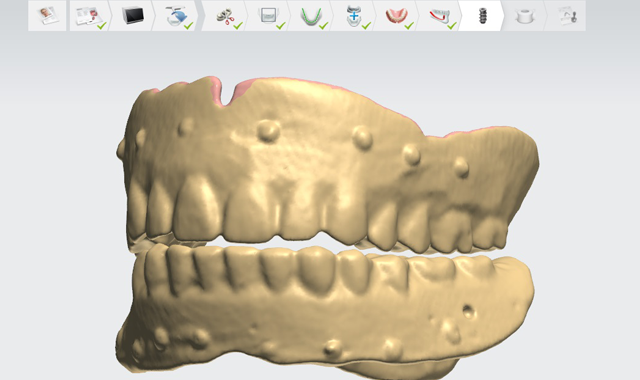
Fig. 5 Second scan of individual denture appliances.
A second scan was made of the individual denture appliances themselves. (Fig. 5) The radio opaque markers are used as landmarks to merge the two scans together.

Fig. 6 Three-dimensional virtual model of the patient.
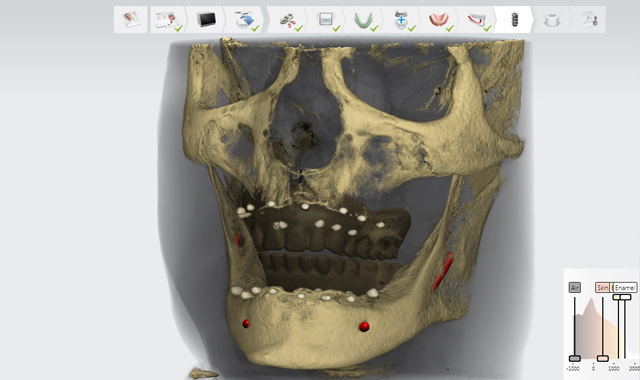
Fig. 6 Three-dimensional virtual model of the patient.
Using the Implant Studio software, a 3D virtual model of the patient was created. (Fig. 6)

Fig. 7 Model of the patient with implant locations.
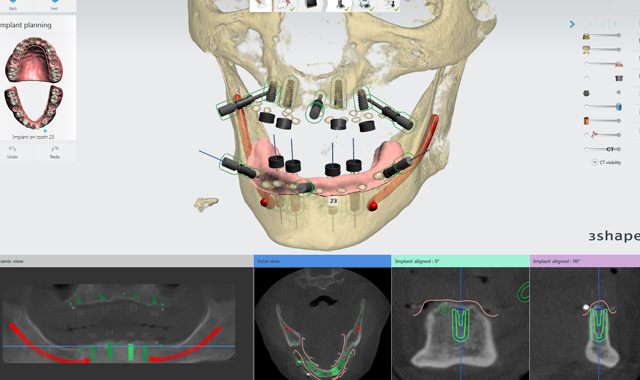
Fig. 7 Model of the patient with implant locations.
A live online planning session was conducted with Dr. Kooner. During this session, the fact that the patient had experienced moderate bone loss due to being fully edentulous for many years was noted, and the appropriate size and length of implants were chosen and placed in the best possible locations for success. (Fig. 7)

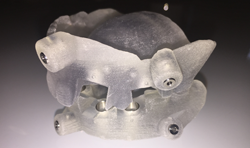
Fig. 8 Finished surgical guide.
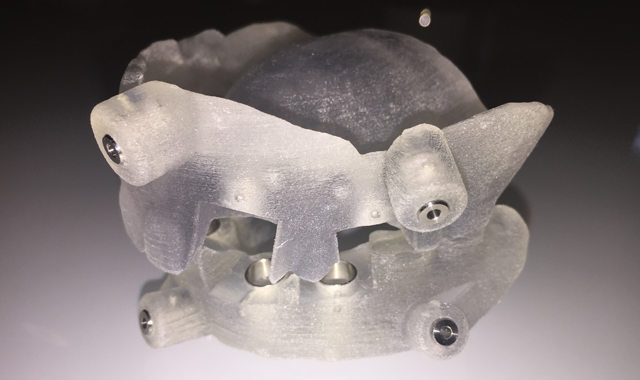
Fig. 8 Finished surgical guide.
The surgical guides, one for the maxilla and one for the mandibular, were designed and fabricated using 3D printing technology by Core3dcentres®.
It is important to note that no physical models were ever produced. The guides themselves were a digitally accurate reproduction of the patient's existing dentures with drilling sites added to facilitate surgery. (Fig. 8; only one pictured) The guides were then shipped to the doctor's office with the required parts to perform the surgery. The surgery itself was an absolute success. In Doctor Kooner’s own words:
Related: How Core3dcentres helps labs meet new challenges
“Patient John S. underwent placement of eight implants in the maxilla and mandible with the aid of a fully guided surgical stent. The stent was planned in advance with Jason Atwood of Core3D in a digital platform. The implants were virtually placed with both surgical and restorative considerations taken. This process minimizes surgical complications and ensures a prosthetically-driven final restoration. It was the best kind of dental implant surgery-uneventful. The patient tolerated the procedure extremely well with only the use of local anesthetic and oral sedation. Moving forward, I would not consider full arch dental implant surgery without the assistance of fully guided stents.”
I am happy to report that the patient is doing well with his implants. They are buried and integrating; and should be ready to restore on schedule. The plan is to do fixed full-arch prosthesis on four implants in each arch, based on the same dentures that the patient has been happily wearing for many years. The difference is that the lab technician was involved in the whole restorative process, and not just the fabrication of the final prosthesis. The implants were planned and placed with the location of the final restorations taken into consideration. Now, when the case comes to the lab, they already have a digital guide to use as a template for the restorations.
News: Core3dcentres' new digital certification program goes live
This use of digital technology makes results consistently predictable. Involving the lab technician from the beginning is like handing them a map before they get into the driver’s seat-or using GPS while driving. For the technician, there is no longer a need for self-navigation or to ask for directions. For the Dentist, a lab technician well trained in digital technology becomes a valuable resource.
When I see what the dentist and technician can accomplish working together in a digital environment, I am reminded of a quote often mistakenly attributed to Albert Einstein:
“Computers are incredibly fast, accurate and stupid. Man is unbelievably slow, inaccurate and brilliant. The marriage of the two is a force beyond calculation.” -Leo Cherne










