New study reports dental care turnout is low among pregnant women
The report found despite dental care being recommended for women throughout their pregnancies, turnout for care remains low.



The BMC Oral Health Journal published a report on the dental health of women during pregnancy. Authors Chandni Muralidharan and Ray M. Merrill, both from the Department of Public Health, College of Life Sciences at Brigham Young University, based their findings on the Pregnancy Risk Assessment Monitoring System in Utah (Utah PRAMS), a surveillance project for the Centers for Disease Control and state health departments.
The Results
Muralidharan and Merrill found despite dental care being recommended for women throughout their pregnancies, turnout for care remains low. This analysis was based on 2,793 women’s responses to the 2014-2015 Utah PRAMS survey, most of whom were in the 21 to 30-year-old age range.
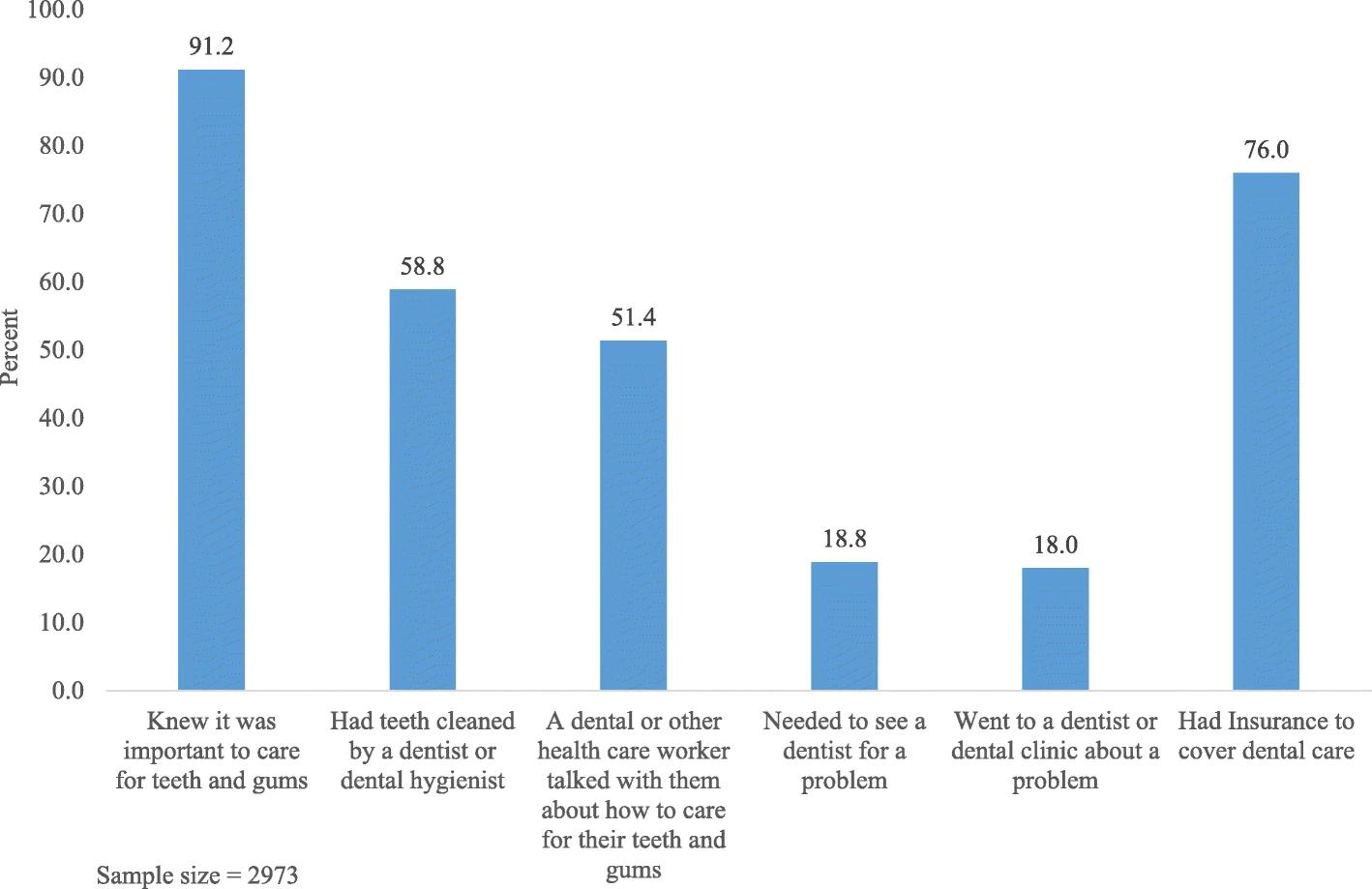
They found 91.2 percent of respondents knew it was important to care for their teeth and gums during pregnancy. However, only 58.8 percent actually had their teeth cleaned while pregnant. What’s more, women who reported knowing of the importance of oral health during pregnancy were only 1.4 times more likely to have their teeth cleaned.
The Reasons
About 76 percent of soon-to-be mothers studied had dental insurance at the time of the survey, meaning they were 1.9 times more likely to have their teeth cleaned and 1.6 times more likely to receive necessary treatment. These findings suggest health or dental insurance coverage played a role in a woman’s decision to visit a dentist, the report concludes.
Additionally, the type of insurance a woman has played into that decision as well, Muralidharan and Merrill state. Pregnant women with private insurance or Medicaid are less likely to visit a dentist when compared to their non-pregnant peers. A PRAMS study indicates women with Medicaid are 24 to 53 percent less likely to receive dental care than those with private insurance.
“This is particularly concerning since Medicaid insurance for dental care during pregnancy, as it is available in most states, only provides coverage during their pregnancy and for 2 months postpartum, such that if dental care is delayed because of pregnancy, there may not be insurance to cover treatment later on,” Muralidharan and Merrill report.


Dental care during pregnancy based on the pregnancy risk assessment monitoring system in Utah
Demographics groups, too, had an effect on the failure to receive oral care during pregnancy, as did behaviors like smoking and alcohol consumption. Pregnant women who are younger, unmarried, lower-income, and have a lower education are less likely to get dental care during pregnancy, the report stated. The same is true of women who smoke cigarettes and drink alcohol. However, Muralidharan and Merrill point out it’s difficult to know a whole lot about the characteristics of the women who are insured.
But insurance coverage and demographic characteristics weren’t the only factors, Muralidharan and Merrill say. The study states some dentists and obstetricians contribute to the lower turnout of pregnant women in dental offices. The report cites a study in which only 40 percent of women were advised by their obstetric provider to receive dental care during their pregnancy and 10 percent were refused oral care by their dentists during pregnancy. Another survey found 73 percent of gynecologists mistakenly believed dental x-rays were unsafe for pregnant women, while 58 percent believed the same of local anesthesia.
In addition, some healthcare providers are not advising their patients about the importance of receiving dental care during pregnancy, the report states. Only 41 percent of pregnant women received oral health counseling, according to a 2004 to 2006 PRAMS study involving 10 states. Yet, Muralidharan and Merrill say, more research is needed to understand if receiving such counseling has any effect on a woman actually making an appointment and being seen by a dentist.
“Many dental and obstetrics workers may simply be unaware of the prenatal oral health guidelines, thereby causing them to not recommend dental care during pregnancy and to be less likely to talk with their patients about how to care for their teeth and gums during pregnancy,” the BMC report says.
Why it Matters
“During pregnancy, a woman’s body goes through several changes that can cause oral health problems, including hormonal changes, fluctuation in oral hygiene practices and eating patterns,” the report says. “Poor dental hygiene and gum disease can increase the risk of heart attack, stroke, and adverse pregnancy outcomes.”
The report cites a 2012 national experts’ consensus that concluded dental care was safe and research supports “that routine preventive, diagnostic, and restorative dental therapy, and periodontal treatment, among pregnant women, does not increase the risk of adverse pregnancy outcomes,” Muralidharan and Merrill write. What’s more, continued dental care during pregnancy is important to avoid periodontal disease, which can result in pre-eclampsia, preterm birth, and low birth weight, the report says.
According to the American Academy of Periodontology, research supports this statement-women with periodontal disease could be more likely to deliver prematurely or give birth to newborns with a low birth weight compared to mothers with healthy gums. A birth weight less than 5.5 pounds could bring a number of health concerns such as delayed motor skills, learning disabilities, respiratory problems, vision and hearing loss, or feeding and digestive issues, according to the CDC.
Several educational programs are in place to increase patient use of dental services during pregnancy, the report says. These efforts include Integration of Oral Health and Primary care Practice, an outline of inter-professional core clinical competencies for oral health to be implemented by primary care providers, which was released by the Health Resources and Services Administration, part of HHS. A course called Smiles for Life: A National Oral Health Curriculum, contains material designed for pregnant dental patients, the report says.
The BMC-series Journal is a collection of peer-reviewed articles covering all scientific and medical disciplines. For more information, visit biomedcentral.com/p/the-bmc-series-journals.










