How is dental technology REALLY being used?
Digital Esthetics surveyed the dental industry to find out how technology is really impacting dentistry. Here's what we found.

CAD/CAM and digital dentistry are major forces driving the industry, but to what extent? To find out, Digital Esthetics conducted a survey to determine how technology is driving dentistry. The survey asked respondents about how they utilize technology, what kinds of equipment they use and how they interact with their lab or doctor.
The survey included 330 respondents-114 from labs and 216 from dental offices. Some of the major demographics include:
Labs
- 75 percent of respondents are lab owners
- 80 percent have been in the field for more than 20 years
- 44 percent work in labs with one to three employees, 17 percent work in labs with four to six employees
- 43 percent of the labs perform crown and bridge work while 35 percent are full-service labs
Dental offices
- 76 percent of respondents are dentists and the practice owner
- 77 percent have been in the dental field for more than 20 years
- 36 percent are in practices with one to three employees, 35 percent are in practices with four to six employees
- 78 percent are general dentists
- 64 percent send their cases to a local lab, while 21 percent send to a national lab
Using intraoral scans

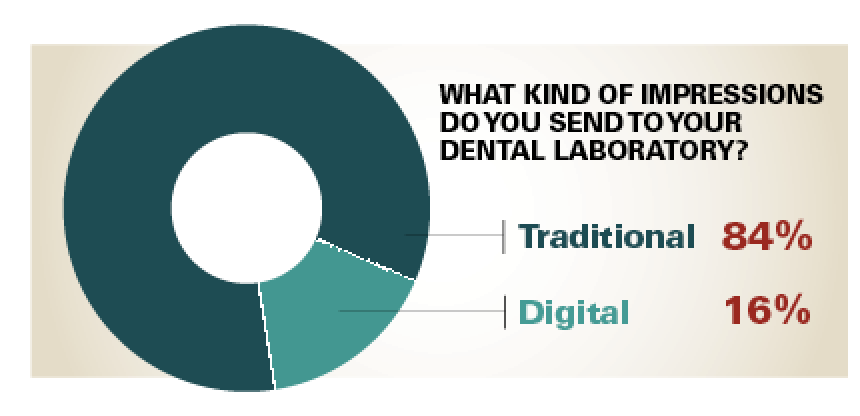
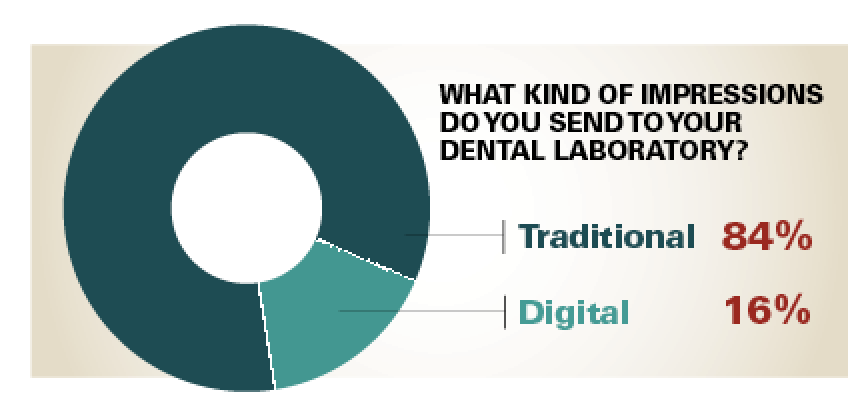
About 16 percent of labs report using intraoral scans from their doctors, yet 30 percent of doctors report owning intraoral scanners. The data also show that many doctors are milling their restorations in-house.
Mark Ferguson, General Manager, Vulcan Custom Dental, looks to the types of equipment that doctors are using.
“A good amount of them are using CEREC,” Ferguson notes. “That, right there, eliminates the lab work.”
But others may simply not use the scanners, even after they’ve been purchased.
“You’re always going to have a few people who want to jump and get something, and for whatever reason, after they get it, they don’t like it,” says Dr. John Flucke, DDS, Technology Editor for Dental Products Report. “I’ve always been of the opinion that if I can’t make something work, I always think to myself, ‘There are people out there who are doing this and they’re making it work.’ So I tend to push myself until I finally get the grasp of it. But some people get frustrated, and they also don’t want to give an appearance of being baffled in front of their patients, and so it just becomes a thing that it’s easier not to deal with it. Put it in a corner and put a potted plant on it.”
“They’re just not using it,” adds Dr. David Rice, DDS, a general dentist in East Amherst, New York. “They purchased the technology, and whether it’s fear of the technology, inadequate training or they just haven’t had success with it; they purchased it and they’re just not using it at all.”
Chairside trends
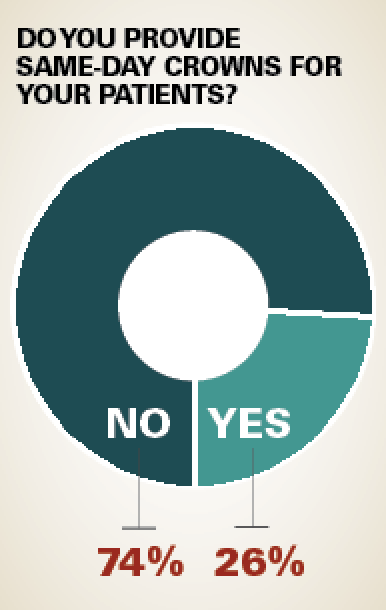
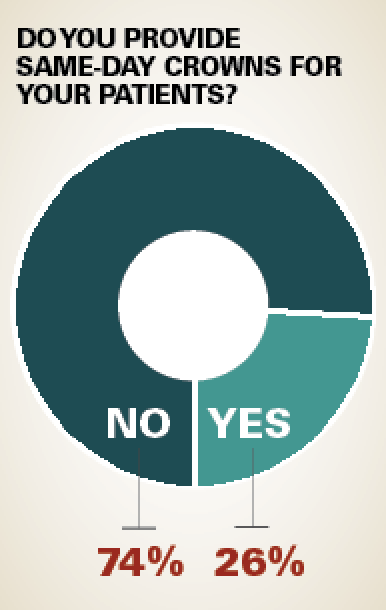
About 27 percent of respondent doctors indicated that they own chairside milling machines. Those doctors are leading the way into territory that many believe will be the future of dentistry.
“Today’s patient is starting to demand efficiency,” Dr. Rice says. “People are busier than they have ever been, and the 45-and-under patients know that technology exists. They are more and more demanding of that technology. They don’t want to wear a temporary. They don’t want to come back twice. They don’t want to be numb twice. They want life to be simple.”
Dr. Flucke’s experience with chairside milling was hit-or-miss, but the quality has improved over its initial iteration and promises to only get better and less expensive.
“The outcomes weren’t as predictable as they are now,” Dr. Flucke says. “Nowadays, the same-day stuff is really predictable. I would be going along just fine, but then we had a couple of cases that we just couldn’t make it work at all. We’d get things out of the machine that looked like it was meant for somebody else, and we just couldn’t use it.”
Dr. Flucke observes that dentists who are now graduating from dental school will especially embrace chairside, but they have their own obstacles to overcome.
“The people that are graduating now have such a greater comfort level with digital,” he continues. “I think it’ll grow. The one limiting factor, of course, is always going to be money. You’ve got to have a decent amount of cash to get one of these. I used to think the big thing that held people back was fear of the technology, and I don’t really feel like that’s a limiting factor now. There are a lot of younger dentists who could do it in a heartbeat and not have any problem with it, but those folks are fairly heavy in debt from education. When you get out of school and you’re $275,000 in debt, and if you want to purchase a practice or open a practice, that’s more money, and then you want to have same-day crown or an onlay device in your office, that’s another outlay of six figures. But they are amazing devices, I’ll say that. They produce amazing, amazing restorations.”
Design work
Of the doctors that perform chairside and in-house restorations, the survey revealed that the doctors, themselves, performed the design work 83 percent of the time. But it is a task that can readily be performed by another trained member of staff.
“You can have another staff member do it easily,” Dr. Flucke says. “For some dentists, because we’re so hands-on and so perfection-oriented, I think some doctors have this attitude of, ‘It’s not right if I don’t touch it.’ ”
When Dr. Flucke offered chairside services, he gave the duty to another staff member.
“I had a couple of staff members who were very well-trained in it, and they could do a lot of them on their own,” Dr. Flucke says. “But there was the occasional one where they had a question on something, and they would come get me, and I would plunk down really quickly to make a change, or look at something and say, ‘No it’s good, you got it,’ but I didn’t do all those myself, by any stretch of the imagination.”
Some of the doctors’ decisions to perform the design work, personally, might also be due to local rules and regulations.
“It’s not that it’s against the law or against code, but some states are more strict than others when it comes to how they manage things,” Dr. Rice says. “So some dentists, in general, shy away from the expanded duties on the assistant’s side. People should be engaging their team in the process. One, from an efficiency standpoint, and two, from an empowerment of their team standpoint. If you can get your team feeling like they are really truly a part of important processes instead of menial labor, you tend to get a higher caliber of team member and retain them.”
Outsourcing milling
When asked about what types of equipment labs own, an interesting result was that 53 percent reported owning a sintering furnace while 50 percent own a mill. It raises the question: What are those other three percent sintering?
Ferguson observes that those labs are likely outsourcing their milling and completing the cases when they come back to the lab.
“I think it’s absolutely a smart way to go for dental labs,” Ferguson says. “They can outsource the milling and the problems associated with milling. All of a sudden, now they’re really taking control of the final product-even without the milling machine.”
Outsourcing milling is a good option for labs that don’t want to invest in a mill or that want to be part of the digital workflow.
“They have doctors that are getting intraoral scanners and sending digital cases to them, but they don’t have a digital solution in-house,” Jason Atwood, CDT, Senior Digital Solutions Advisor, Core3dcentres says. “So they need a milling center to help them out. Some labs have a scanner or a small mill, but can’t handle some cases, and they use us as a milling center for that.”
Atwood references a local lab that does not own milling technology, but as their doctors embrace digital, they send the cases to Core3dcentres for milling. It is a win-win-win relationship.

“It’s a good relationship for him, because he is a small three-person lab, and he doesn’t do enough volume to justify investing in a milling machine and some of these high-tech devices,” he says. “So he’s willing to just pay case-by-case so he can keep that relationship with the doctors that he has, as they embrace digital technology and send him cases.”
“It’s an intermediate step where you can kind of dip your toe in and then slowly go in the water, rather than cannonball in the deep end,” Ferguson says.
Equipment costs
Not surprisingly, both labs and doctors tend to own less expensive pieces of equipment (like lasers and benchtop scanners) than the more expensive pieces of equipment (like cone beam scanners and SLM machines), and the decision when one may buy more expensive equipment is based on a number of factors.
“A lot of it is perceived value,” Ferguson says. “To get a printer that was accurate enough to print models, a dental lab was looking at over $100,000. Most labs are going to say, ‘Am I going to spend $100,000, or am I going to pay $25 a model? I’ll pay $25 a model.’ ”
There is perceived value for milling machines.
“With the dental milling machines you have half of the respondents saying, ‘Yes,’ ” Ferguson says. “There is perceived value there. I can spend $35,000 and buy a mill, and now all of a sudden, I’m going to buy a disc of zirconia for $100, and I get 20 units per disc, each unit is going to be $5. Well, without investigating any further, which a lot of lab owners don’t do, they say, ‘I’d rather do that than spend any other higher price.’ So there is a perceived return on investment almost immediately in that their outsourcing bill is going to go down for zirconia.”
Dr. Flucke notices a specific price point where doctors tend to think more critically about their purchase.
“I have noticed, in my time in dealing with doctors, that $5,000, for some reason, is this magic number,” Dr. Flucke says. “If something is $5,000 or less, and the doctor wants it, he’ll buy it and not really blink. If it goes over that $5,000 mark, that’s when the doctor starts saying, ‘Well, I have to talk to the accountant. I’m going to really need to think about this.’ It’s not just a, ‘Throw the credit card down,’ and say, ‘Yeah ship one to my office,’ sort of thing.”
As technology and equipment matures and spends some time in the marketplace, costs tend to come down and it becomes more accessible to more doctors and labs.
“For sure cost is a factor, because the technology is still quite new,” Atwood says. “Milling machines have actually come down in price significantly since they first came on the market. They have the smaller desktop milling machines now. They do a fair job and are much more affordable.”
“There are some 3D printers now that are extremely reasonably priced,” Ferguson adds. “As they get vetted through the early adopters, they may end up being far more commonplace than even the milling machines.”
Next page: Are both old and young dental professionals using digital tools? Here's what you told us ...
Issues of age
Respondents’ ages told some interesting tales.
Most of the survey respondents (68 percent of labs and 67 percent of dental offices) were Baby Boomers. Generation X represented about 21 percent each.
For Ferguson, it was impressive that more than 80 percent of respondents have been in the dental field for more than 20 years but are still willing to embrace digital.
“To see that there were a decent amount of people who were incorporating digital into their lab or into their office is really exciting,” Ferguson says. “Traditionally that’s been one of the issues, particularly on the clinical side. What ends up happening, clinically, is dental students are taught by older dentists who don’t want to learn new technology just to teach it. Dental schools now are starting to embrace technology. For a number of years labs felt like we spent all this money on digital, but our doctors don’t know or don’t care. What I’m seeing a lot more now is that doctors do care, beyond bringing an in-house milling unit into their office to eliminate the lab. I think it’s now how can we work with the lab for a better patient experience.”
But not everyone is embracing change with as much enthusiasm. One of the Baby Boomer respondents made this comment:
“There is an uneasy feeling giving up technique and touch to a software,” the respondent writes. “Relying on tech support is another fairly uneasy situation. Being a Baby Boomer, the digital learning curve and becoming proficient with not only the CAD and CAM software, but also the operating systems, importing, exporting, moving and transferring files is daunting.”
Generation Y and Millennials represented just four percent of dental offices and eight percent of labs. That demographic is largely seen as one that embraces technology and is expected to drive change.
“Change is really difficult for many people, especially people in dentistry,” Dr. Rice says. “Dentists, in general, find a place where things are working, and it is difficult for them to rationalize shifting gears. Unfortunately, with the Millennials hitting the marketplace, it’s going to be a necessity for them to shift gears.
“I work with a ton of millennial dentists,” Dr. Rice continues. “What I see in them is that digital imaging is absolutely a part of their immediate future. In some way shape or form, digital impressions, digital scanning, soft tissue lasers, and-if you are either a go-getter, a general practitioner, or a specialist-cone beam is part of your standard of care.”
What labs love about digital
Lab owners responded that digital materials (like zirconia or millable lithium disilicate) are faster to work with (69 percent) and easier to finish (50 percent).
To the list of advantages, Atwood adds accuracy.
“One of the things that we noticed, because we do high volumes, is that digital impressions and digital models have fewer remakes for fit issues than traditional impressions,” Atwood says. “That’s a big deal. As long as you’re working with high-quality equipment, the accuracy is much better than traditional methods.”
Ferguson observes that digital processes make life easier for the technician.
“Digital is certainly a faster way, not necessarily to get the product out the door, but just in terms of technician labor,” Ferguson says. “By offloading some of the labor onto a machine, it is a really helpful thing. I can design a certain number of units and let a machine mill them overnight, rather than wax a bunch of units, invest them, press them and spend overnight with them. Labor hours certainly become a factor in there but, for me, I look at digital as a new tool. I got into digital because we were milling materials that couldn’t be fabricated any other way. We were kind of, for lack of a better term, forced into it. But through that, I think that we’re still in the infancy of CAD/CAM. As we’ve seen with zirconia and progressions from bright white zirconia to far more esthetic zirconia nowadays, I think we’re going to see evolutions in all areas.”
Additional comments on digital dentistry from laboratory respondents include:
“I think digital dentistry still needs to improve, esthetically, to show more variation in depth. More time needs to be taken in training computer specialists in the design and fit of crowns. The machines aren’t to the point where they can just have the crowns milled and sent out without some checking on fit and look.”
“Options are greater with a digital workflow. We have to be careful not to neglect traditional techniques when going digital. Mounting cases on adjustable articulators and verifying occlusion is still critical. Virtual articulators are getting better, but can’t resolve all the issues. We can’t just rely on digital!”
How doctors regard digital materials
Doctors cited strength and ease of use as their biggest draws to digital materials.
For example, the majority of Dr. Flucke’s crowns are lithium disilicate and he uses zirconia when he needs strength.
“The lithium disilicate is just so esthetic,” Dr. Flucke says. “It is just gorgeous. It is a rare occurrence now for me to get something back, and go to put it in the mouth, and say, ‘Oh, it just doesn’t look natural.’ The lithium disilicate is one of those things where sometimes you look at it and say, ‘Is that real?’ We actually have to stop and take a second look before we realize that, ‘Yes, that’s a crown.’ ”
Dr. Rice also lauds lithium disilicate and its virtues.
“In my humble opinion, one of the weakest areas in dentistry is an understanding of materials,” Dr. Rice says. “Lithium disilicate is the most time-tested and durable material that we’ve seen that strikes a balance between strength, being gentle, and being kind to the adjacent and opposing teeth. And on top of that it’s a retrievable material.”
Zirconia, on the other hand, he sees as being pushed on dentists.
“I’m not a great fan of zirconia,” Dr. Rice observes. “It’s cheap to manufacture, it’s less expensive for labs to manufacture, so there’s a lot more profit margin for the material, and the market is really driving the dentistry, instead of the dentistry driving the market.”
Some of the respondent doctor views on technology included:
“Digital material is not just easier to work with for the dental technician, but also way easier for dentists. When some adjustment is required in the mouth, no worries when grinding down, because of durability of the material. In contrast, traditional restorations, when adjustment in the mouth required, often comes with the cracks, crushing and destruction of the porcelain.”
“If the digital fabrication of crowns is done carefully and skillfully, it is equal in quality to carefully and skillfully made traditional crowns. Sometimes those that are digitally made are too loose, no natural retention of crown on tooth.”
“I’ve seen some pretty crappy ‘digital’ dentistry as well as traditionally produced products. It’s more about the dentist’s skills than the toys.”
The state of digital dentistry
The survey gave some interesting insights into current thoughts and usage of digital dentistry by both labs and clinicians. It is a modality that is likely to persist and evolve.
“I think it’s here to stay,” Atwood says. “I think it’s going to take over. We are on the cusp of going completely model-less with dentistry. I remember the first time I went and sat in a dentist’s office and he had an intraoral camera, and it didn’t actually take any scans, it just let you see the inside of the mouth. It was a neat little toy. It wasn’t really very useful, but it opened up the door for this new technology that’s coming out, and instead of trying to take a traditional impression, and gagging, and trying to keep your mouth open, they can use a digital camera. It’s quick, it’s easy, it’s less intrusive, and it’s more accurate when done correctly. As the milling side of things gets more and more predictable, the accuracy of the digital is going to allow us to go model-less. You’ll be able to scan a patient in the chair, outsource the crown, bring it back and place it in the patient’s mouth without ever trying it on a model. I think that’s going to be your everyday dentistry in the next five to 10 years.”
Dr. Rice expects digital dentistry to become an enormous influence in the very near future.
“Within the next five-to-seven years, digital dentistry will dominate our profession,” Dr. Rice says. “It’s going to grow at an exponential rate over the next one to two years, because the scanners are getting better and better. There are more scanners coming to the marketplace, so that’s driving more innovation. It’s streamlining the process in the practice on the clinical side. On the business side, as far as patients go, their experience is so much better with digital dentistry than it has been in the past. It’s a matter of time before the physical world of dentistry is passé.”
Dr. Flucke notices a trend in dental technologies, where doctors and labs are now becoming more comfortable with the latest iterations of technology.
“We’re in a period right now where it is more of an adoption phase,” Dr. Flucke says. “It’s not so much of a new device or invention phase. I’m always excited about new things, so I have noticed, in my time in dentistry, that we do go through these phases. There’ll be a lot of innovation and then it’ll take a while for that innovation to improve and then people will get it in their offices. We have an adoption phase, and then companies will go and innovate some more. They can’t saturate the market with new devices or people would get overwhelmed by it, but I think we’re probably getting to the end of the most current adoption phase, and I think were going to see more stuff come out, more innovation. I’m excited about that, because that’s really my bread-and-butter. We haven’t had that in probably 18 months, 24 months, so I’m looking forward to that in the next year or two.”
While there is a lot of exciting technology available to clinicians and labs, Ferguson thinks that the best is yet to come.
“We can look at how far we’ve come with digital,” Ferguson says, “but we haven’t seen anything yet. The workflows are going to get much more streamlined. The tools to raise the level of basic dentistry will certainly get better and better. What’s really exciting is that the tools will get better to raise even a level of high-end dentistry and high-end esthetic and functional lab work. That’s going to become the tipping point, when that’s the focus rather than just if it’s faster or easier. It’s an exciting time to be watching what’s going on, because everything is happening so fast.”










